
Pulmonology — MCQs

On this page
A patient of Scleroderma presents with acute respiratory distress. Chest X-ray shows B/L reticular basilar shadows. What is the next line of investigation in this patient?
A known case of COPD with acute exacerbation of symptoms. On examination patient was conscious and alert, pulse was 110 beats/ min and bilateral wheeze present. All of the following are true in the management of the patient except:
A 60-year male with dyspnea shows honeycombing on HRCT. Labs show positive ANA. Diagnosis?
Best predictor of mortality in pulmonary embolism?
Which finding best indicates poor prognosis in interstitial lung disease?
A 60-year-old male with COPD has FEV1 45% predicted, mMRC grade 2 dyspnea, and 2 exacerbations last year. Which GOLD category?
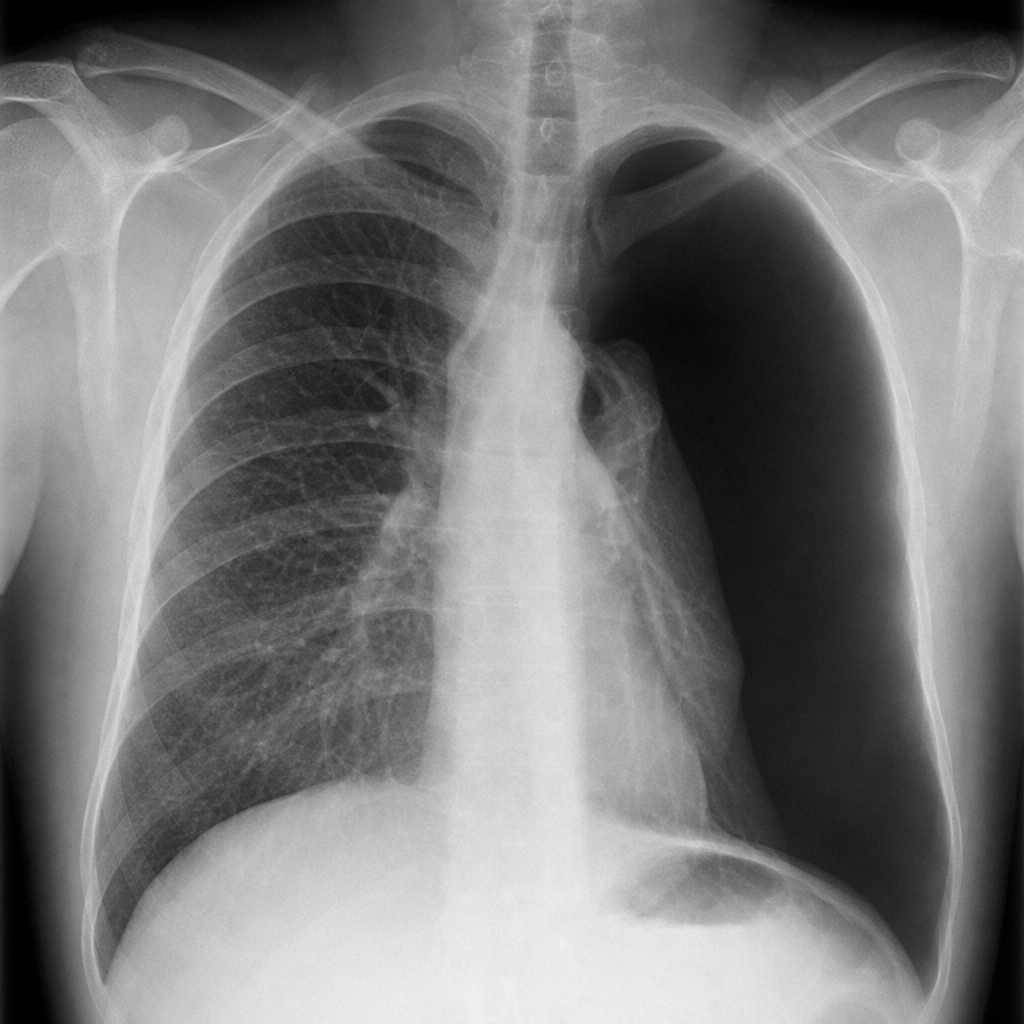
26 year old, 6 feet 4 inch male presented with acute onset dyspnea. On examination, he was tachypneic, other vitals were stable. A chest xray shown absent bronchovascular markings on the left lung compared to right lung with left lung shifted toward the hilum. Most likely diagnosis?
A 45-year-old male presents with chronic cough and shortness of breath. Chest X-ray reveals multiple pulmonary nodules with 'egg-shell' calcification. Which of the following is the most likely diagnosis?
A patient with a history of asthma presents with worsening cough and eosinophilia. CXR shows fleeting infiltrates. Diagnosis?
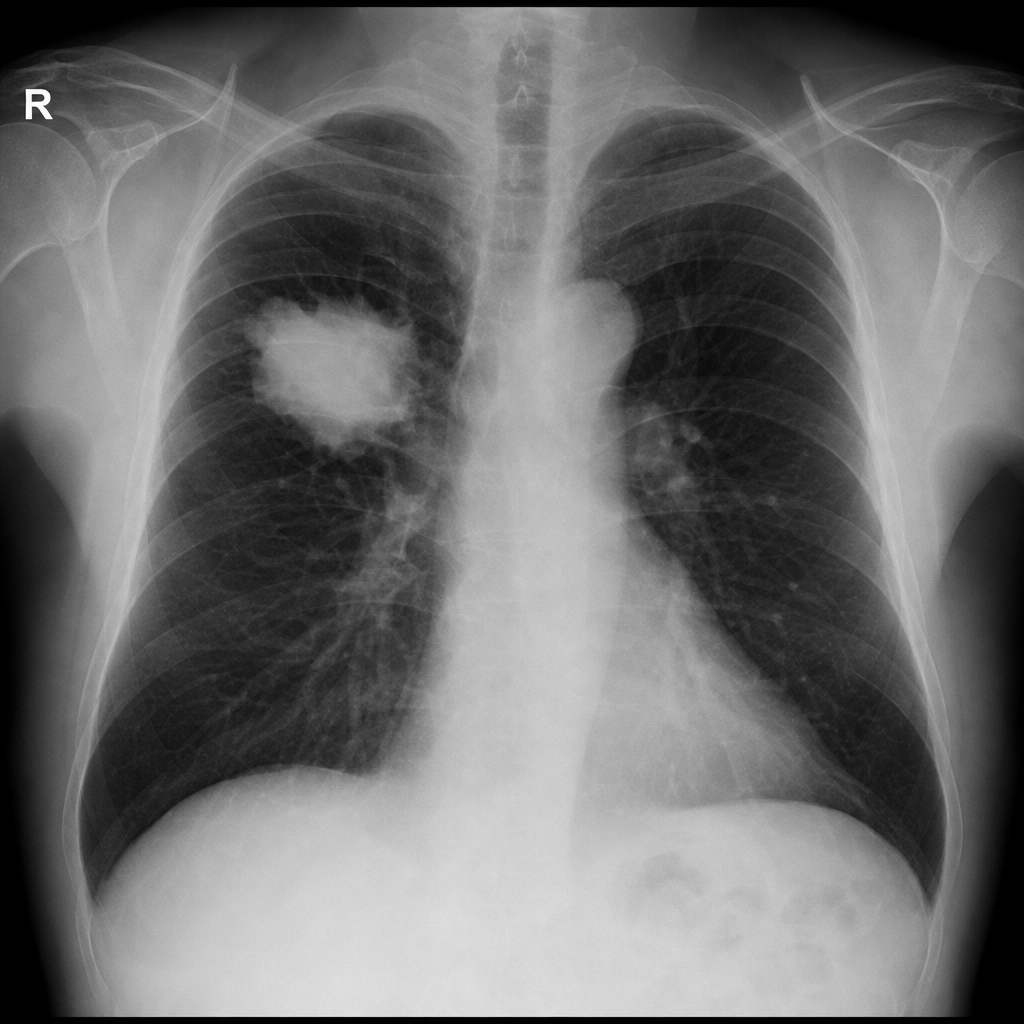
A 70-year-old smoker presents with dyspnea and weight loss. CXR shows a mass in the right lung. Contrast-enhanced chest CT confirms a peripheral lung mass that is safely accessible by a transthoracic approach. What is the next step?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app