
Pulmonology — MCQs

On this page
A 40-year-old male presents with tachypnea. Examination reveals a respiratory rate of 32/min, pulmonary hypertension, blood pressure of 132/90 mmHg, and elevated JVP. What is the most likely cause of these findings?
Which of the following is not associated with pulmonary arterial hypertension?
A 45 year old male, who was operated for fracture of the femur neck, developed severe chest pain, dyspnea, and streaky hemoptysis, followed by hypotension on the 4th postoperative day. The likely etiology is
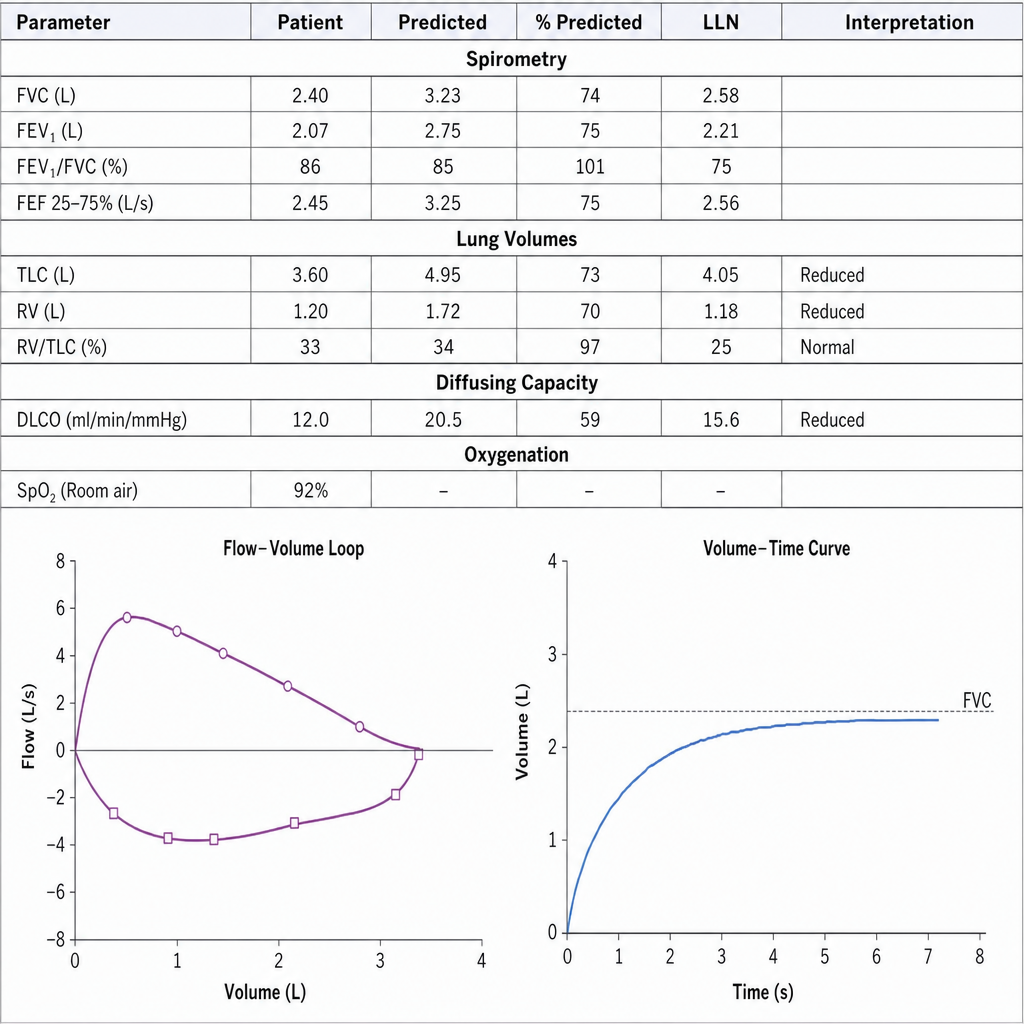
A 28-year-old woman having limited cutaneous scleroderma for the last 10 years complains of shortness of breath for the last one month. Pulmonary function tests (PFT) are as follows. What is the most likely diagnosis in this case?
Which is the investigation of choice for fat embolism?
After a successful Total Hip Replacement a 59 year old patient developed severe chest pain. Echocardiography revealed reduced wall motion of right ventricle with slow flow across the tricuspid valve. Which of the following is most likely diagnosis?
Decreased glucose level in pleural effusion is found in:
A previously healthy 20-year-old man is admitted to a hospital with acute onset of left-sided chest pain. The electrocardiographic findings are normal but chest x-ray shows a 40% left pneumothorax. Treatment consists of which of the following procedures?
Which of the following respiratory lesions is not associated with smoking?
Pack year means
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app