
Pulmonology — MCQs

On this page
A 25-year-old patient presents with acute epigastric pain and elevated serum lipase. The patient was stabilized after 3 days, and a chest X-ray was obtained. What is the most common pulmonary complication associated with this condition?
A patient presents with recurrent lung infections, and the chest X-ray provided shows dextrocardia as a characteristic finding. What is the most likely diagnosis?
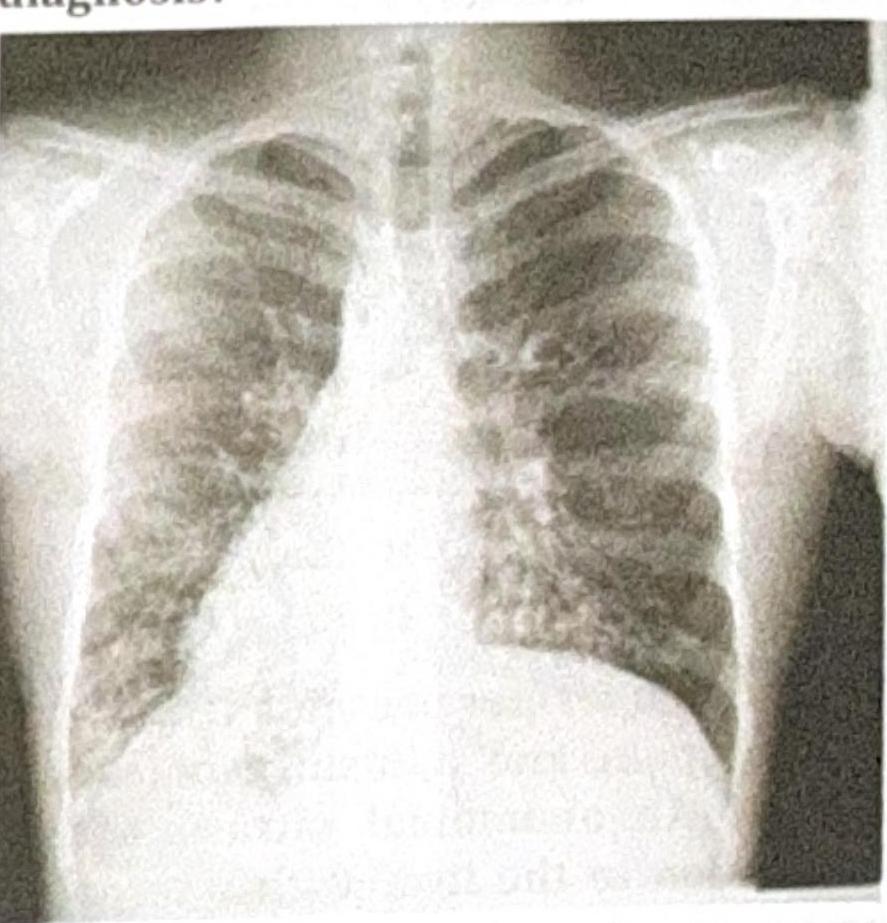
A patient presents with foul-smelling sputum along with breathlessness and fever. Using the X-ray below, identify the diagnosis.
Match the following: A) Caplan syndrome- 1) Found first in coal worker B) Asbestosis- 2) Upper lobe predominance C) Mesothelioma- 3) Involves lower lobe D) Sarcoidosis- 4) Pleural effusion is seen
A 35-year-old female patient with class II pulmonary hypertension presents with a negative vasoreactive test. Which of the following is used in the next step of management?
Six days after undergoing a thoracic endovascular aortic repair following a high-speed motorcycle accident, a 29-year-old woman develops a fever, cough, and shortness of breath. Serum studies show a sodium concentration of 129 mEq/L. An x-ray of the chest shows a left-sided pleural effusion. Thoracentesis is performed and shows milky white fluid in the pleural space that remains uniform after centrifugation. A culture of the pleural fluid shows no organisms. Further analysis of the fluid would most likely show which of the following?
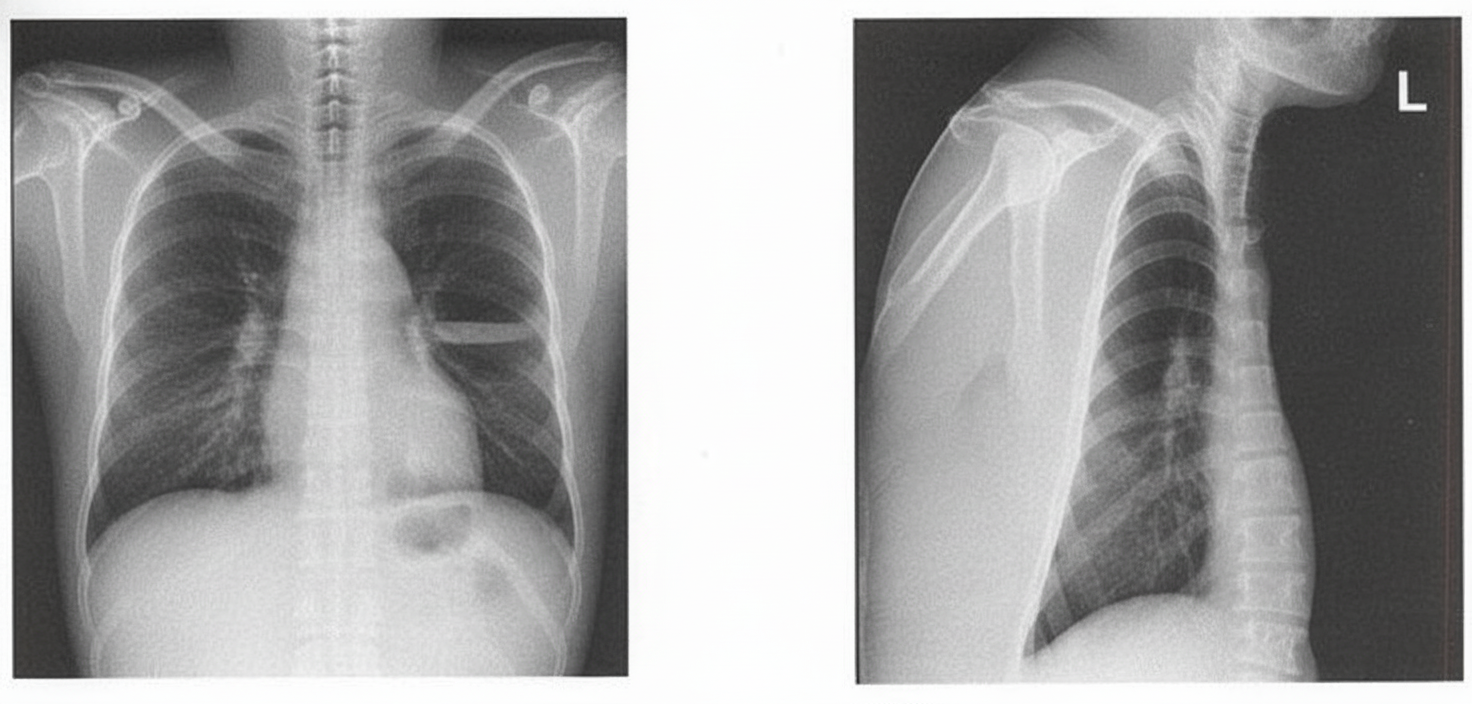
A previously healthy 30-year-old woman presents with 3 months of progressive shortness of breath, nonproductive cough, constipation, and fatigue. Physical examination shows conjunctival injection and tender, erythematous nodules on both shins. The lungs are clear to auscultation. The chest radiograph shown demonstrates bilateral hilar lymphadenopathy. Which of the following additional findings is most likely in this patient?

Which is NOT a feature of pleural effusion?
All are true about Allergic Bronchopulmonary Aspergillosis (ABPA) except?
Irreversible obstructive lung function is seen in which of the following conditions?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app