
Pulmonology — MCQs

On this page
Peri-operative respiratory failure is an example of
Which of the following conditions are contraindications for noninvasive positive-pressure ventilation in patients with respiratory failure? I. Craniofacial abnormalities II. Significant burns III. Respiratory failure with PaCO_2 of 60 mm Hg IV. Cardiovascular instability Select the correct answer using the code given below :
A 62-year old male chronic smoker has been diagnosed with Chronic Obstructive Pulmonary Disease (COPD). On pulmonary function testing, the ratio of Forced Expiratory Volume in 1 second (FEV1) to Forced Vital Capacity (FVC) was 0.6 and FEV1 was 70 % of predicted. What is the severity of airflow obstruction in this patient as per GOLD criteria?
Under the Stepwise Approach to the management of Bronchial Asthma, which one of the following is the correct initial treatment at Step 1 for a patient diagnosed with Asthma?
Consider the following pleural fluid analysis : pH-7.6 Pleural fluid protein -0.5 g / dL Serum total protein -6.5 g / dL Pleural fluid LDH - 100 U / L Serum LDH - 300 U / L What is the most likely diagnosis?
Which organ is PRIMARILY involved in cystic fibrosis?
Consider the following statements: The clinical features of tension pneumothorax include 1. tracheal shift to contralateral side 2. absent breath sounds on the affected side 3. low output circulatory failure 4. peripheral cyanosis Which of the statements given above is/are correct?
Smoking is associated with all the following diseases except:
A 50 year old male presented with pain along the left arm and ptosis. His chest X-ray showed soft tissue opacity at the apex of the left lung along with the erosion of the adjacent rib. The probable diagnosis is:
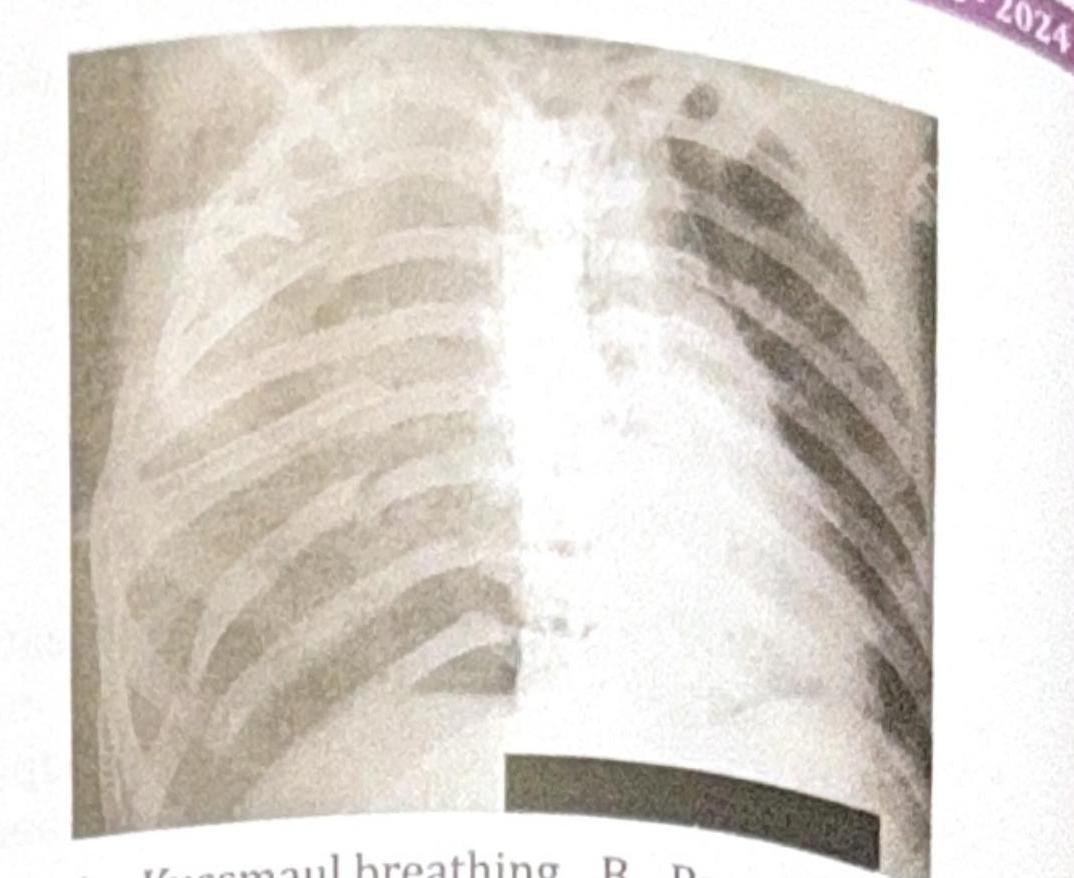
A 45-year-old man presents after a motor vehicle collision with severe left-sided chest pain and dyspnea. He has bruising and marked tenderness over the left anterolateral chest. The initial chest radiograph shown reveals no pneumothorax, pleural effusion, or focal pulmonary consolidation. CT of the chest demonstrates fractures of the left fourth through seventh ribs at two sites along each rib, creating a free-floating chest-wall segment. Which respiratory pattern is most likely observed on inspection?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app