
Pulmonology — MCQs

On this page
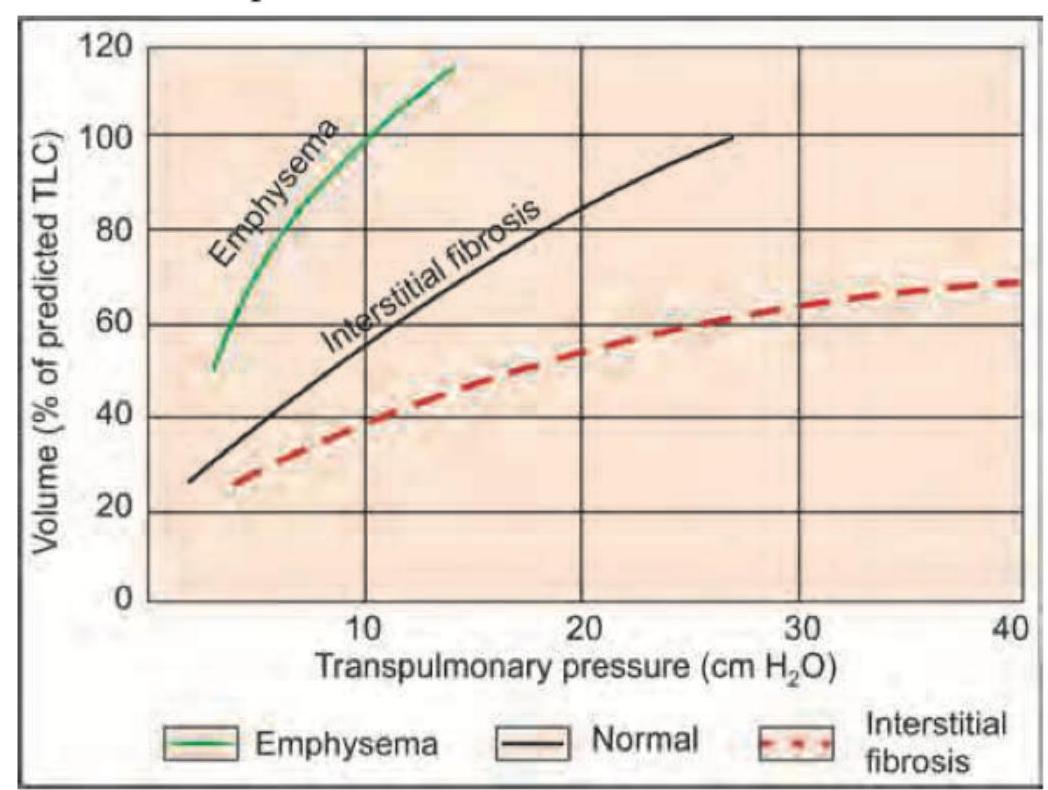
The curve shown is shifted downwards and to the right by which chronic interstitial disease?
Which of the following is seen in the image?
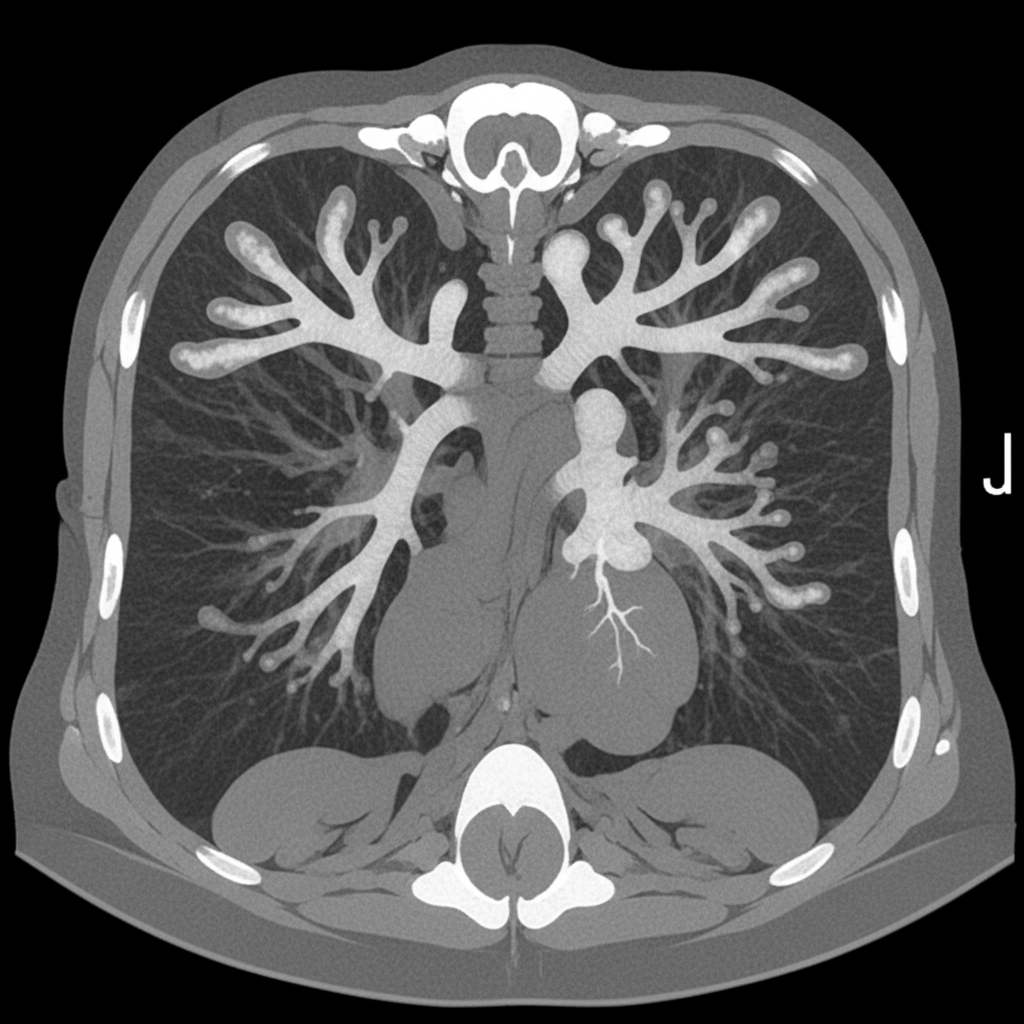
An asthmatic presents with brownish plugs in sputum. CT chest was performed. What is the diagnosis?
A patient of swine flu has developed severe respiratory distress. Which of the following findings confirm the diagnosis of ARDS in this patient?
A 30-year-old patient on respiratory support has a SpO2 of 80% and bilateral crepitations in all lung fields. He was admitted following an episode of aspiration pneumonia, and bedside echocardiography shows preserved left ventricular function. CXR shows presence of:

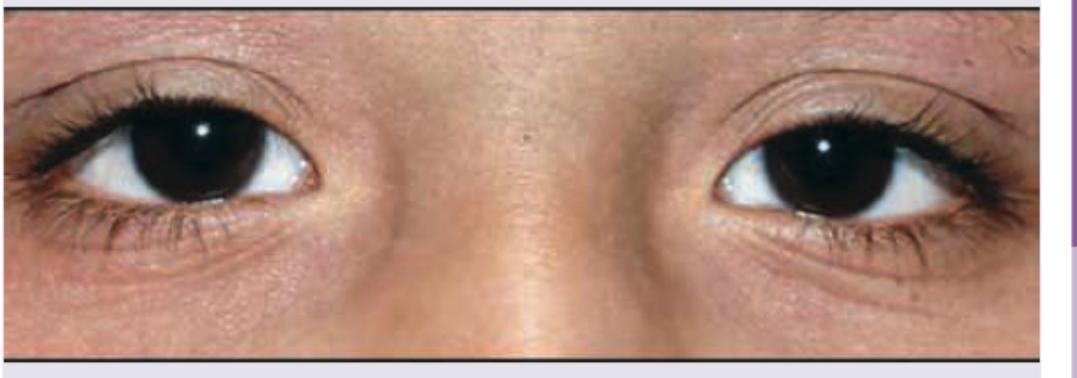
A 35-year-old woman presents with breathlessness at rest. She also complains of a violaceous, indurated skin lesion on nose which has increased in size for last 6 months. What is the diagnosis?
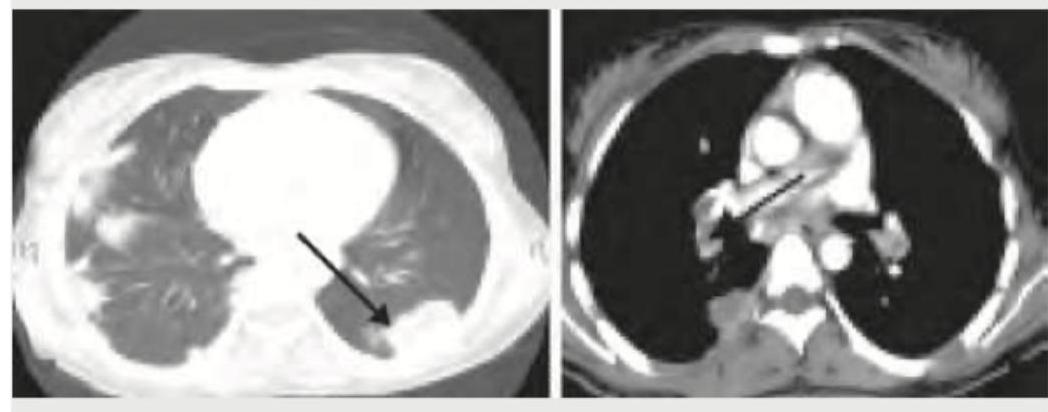
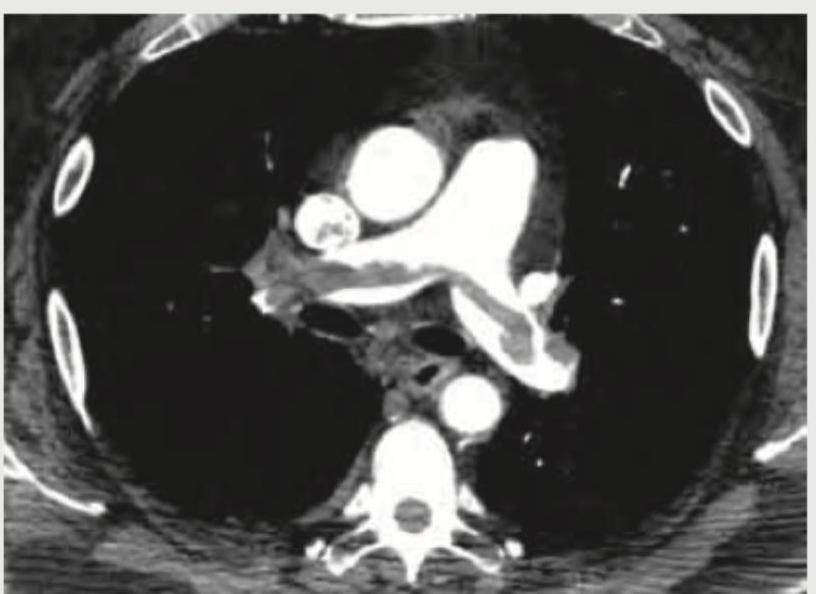
A 30-year-old nephrotic syndrome patient travelled via a non-stop flight from San Francisco to New Delhi. On arrival at the destination, the patient started having difficulty in breathing and was rushed to the hospital. His $\mathrm{SpO}_{2}$ is $85\%$ and ECG shows sinus tachycardia with T wave inversion in lead III. CT chest was performed. What is the diagnosis?
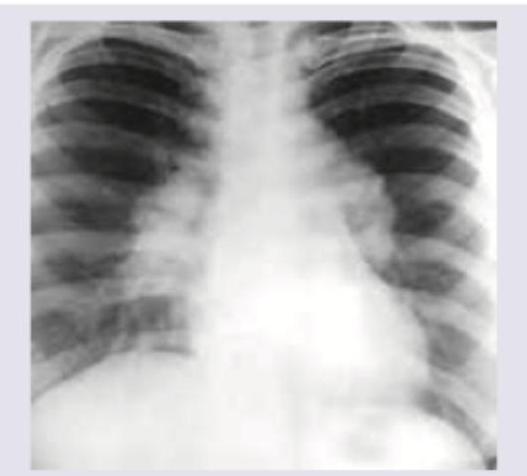
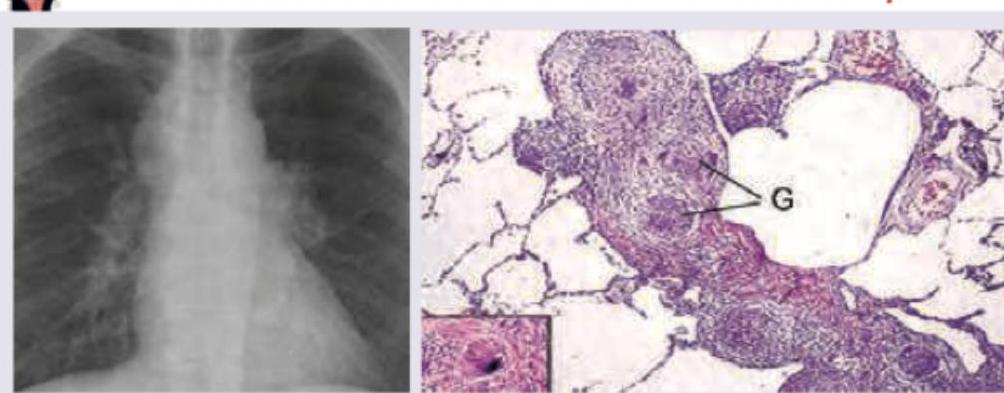
A 35-year-old lady presents with fever, skin rash and dyspnea on exertion for last 2 months. Her chest X-ray is shown below. What is the most likely diagnosis?

A 35-year-old male with history of 4 weeks of immobilization for fracture of femur develops sudden onset breathlessness and blood in sputum. CT angiography shows? (Recent NEET Pattem 2018-19)
All are true about the condition shown except:
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app