
Pulmonology — MCQs

On this page
A 40-year-old man without a significant medical history presents with a 3-day history of fever, shaking chills, and a 15-minute episode of rigor. He also reports a cough productive of yellow-green sputum, anorexia, and right-sided pleuritic chest pain. Shortness of breath has been present for the past 12 hours. Chest x-ray reveals a consolidated right middle lobe infiltrate, and CBC shows an elevated neutrophil count with many band forms present. Which feature would most strongly support inpatient admission and IV antibiotic treatment for this patient?
A 57-year-old male suffering from acute pancreatitis develops sudden onset breathlessness with a CVP < 18 mmHg. The chest X-ray shows bilateral infiltrates. What is the most likely diagnosis?
Superior vena cava (SVC) syndrome is most commonly associated with which of the following conditions?
A 25-year-old male smoker presents with high-grade fever, chills, severe right-sided pleuritic chest pain, and cough with expectoration. Physical examination of the patient is likely to show which of the following?
Type II Respiratory failure is characterized by?
Type II respiratory failure best relates to which of the following?
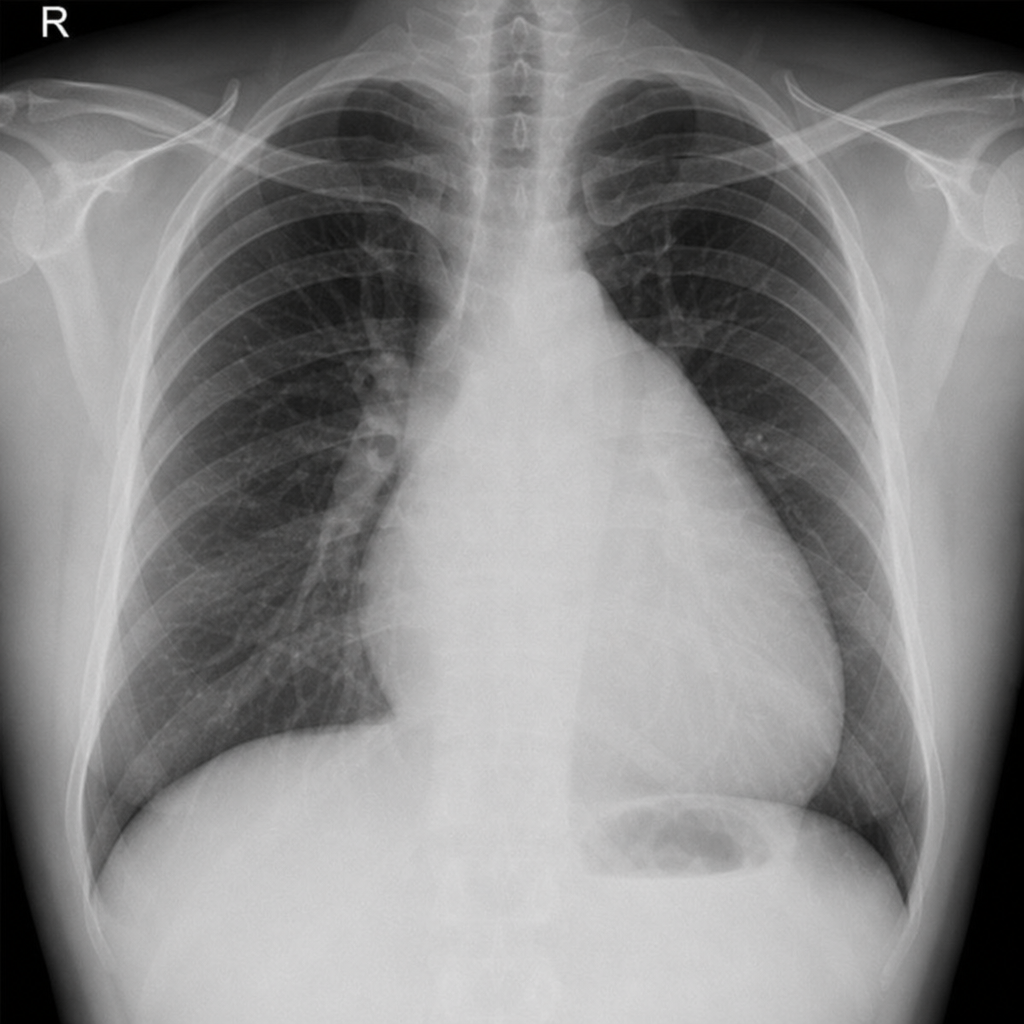
A 45-year-old woman presents with progressive exertional dyspnea, fatigue, and near-syncope over the past year. On examination, she has a loud P2, right ventricular heave, and elevated JVP. Echocardiography reveals right ventricular enlargement and estimated pulmonary artery systolic pressure of 65 mmHg. The following chest X-ray is obtained. What is the most likely diagnosis?
Increased serum amylase in pleural effusion is seen in which of the following conditions?
All the following are radiological features of chronic cor pulmonale except?
Which of the following statements is/are true about obstructive lung disease?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app