
Pulmonology — MCQs

On this page
Which of the following findings is NOT seen in primary pulmonary hypertension?
Clubbing is the least common in which of the following conditions?
A 56-year-old male smoker presents with symptoms of weakness, dizziness, and right chest pain. He reports intermittent pain in the right shoulder and axilla for the past 6 months. He denies exposure to TB and has a negative PPD skin test. Routine laboratory tests are normal. A chest X-ray reveals a right apical superior sulcus mass. What is the most likely associated finding?

A 63-year-old man presents with a 2-day history of cough, rigors, fever, and right-sided pleuritic chest pain. Chest x-ray reveals consolidation of the right lower lobe and a right pleural effusion. Thoracentesis of the pleural fluid shows: Cell count=1110/mm3, Glucose=75 mg/dL (serum glucose=85 mg/dL), Protein=4.0 g/dL (serum protein=7.0 g/dL), LDH=400 U/L (serum LDH=200 U/L), pH=7.35. What is the most likely pathogenesis of this pleural effusion?
A man presented with right-sided moderate-sized pneumothorax without tension. Which physical finding is present?
A 52-year-old businessman with nephrotic syndrome presents with sudden onset of breathlessness, haemoptysis, and chest pain. He is brought into casualty in shock. His chest X-ray is normal and the ECG shows sinus tachycardia. What is the most likely diagnosis?
An 83-year-old man with Parkinson's disease presents with low-grade fever and cough for several weeks. He has been experiencing increased rigidity and difficulty with walking, and is on levodopa/carbidopa. Examination reveals a shuffling gait, resting tremor in the left hand, cogwheel rigidity, and crackles in the left lower lung field. Chest X-ray shows a lung abscess in the left lower lobe. What is the most likely bacteriologic diagnosis for this lung abscess?
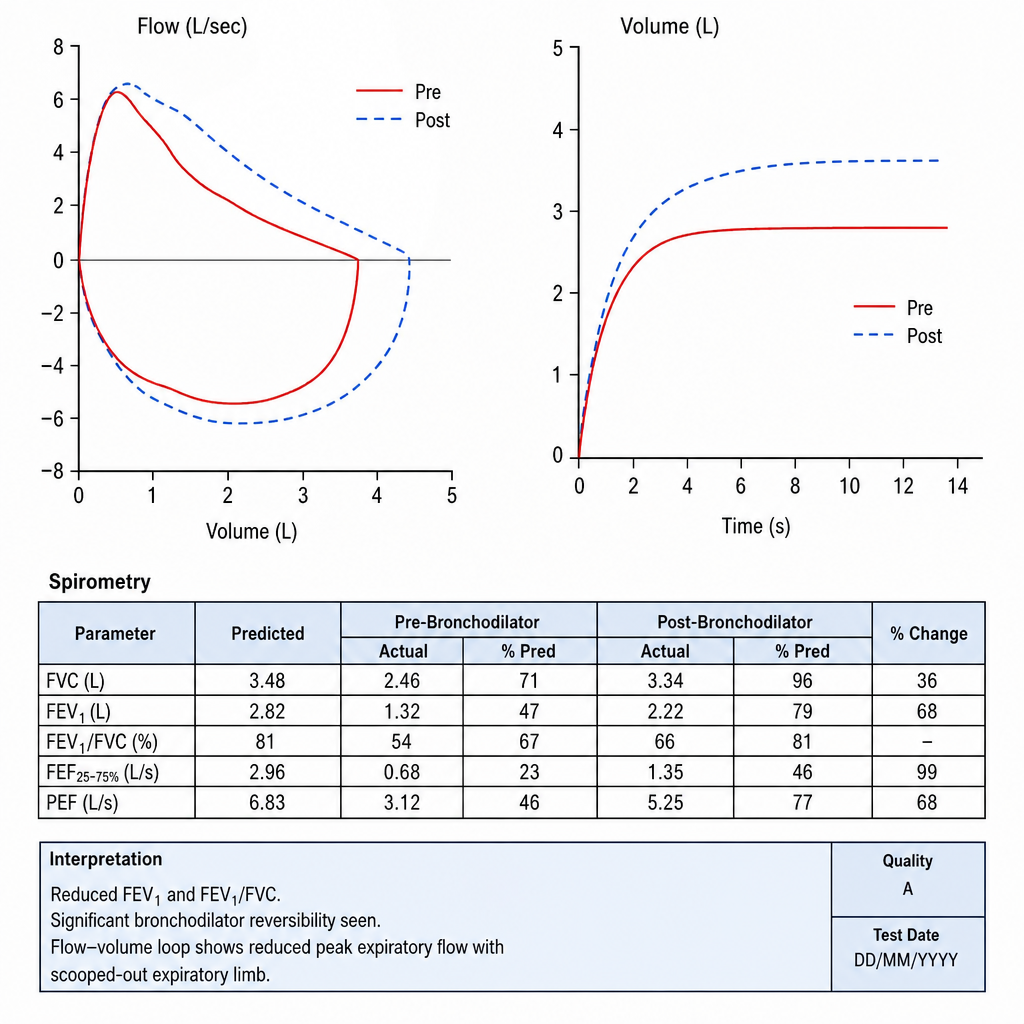
A patient presents with reduced FEV1, normal FVC, and an FEV1/FVC ratio less than 0.7, which is reversible with bronchodilators. This pattern is consistent with which of the following conditions?
The pulmonary function test done on this patient of asthma would be:
What is the drug of choice for the treatment of type 2 Brittle Asthma?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app