
Pulmonology — MCQs

On this page
What is the most common abnormality associated with ARDS?
There is no correlation between X-ray appearance and clinical state of the patient with pneumonia in which of the following etiologies?
What is the initial treatment for pulmonary embolism?
All of the following are causes of hemorrhagic pleural effusion except?
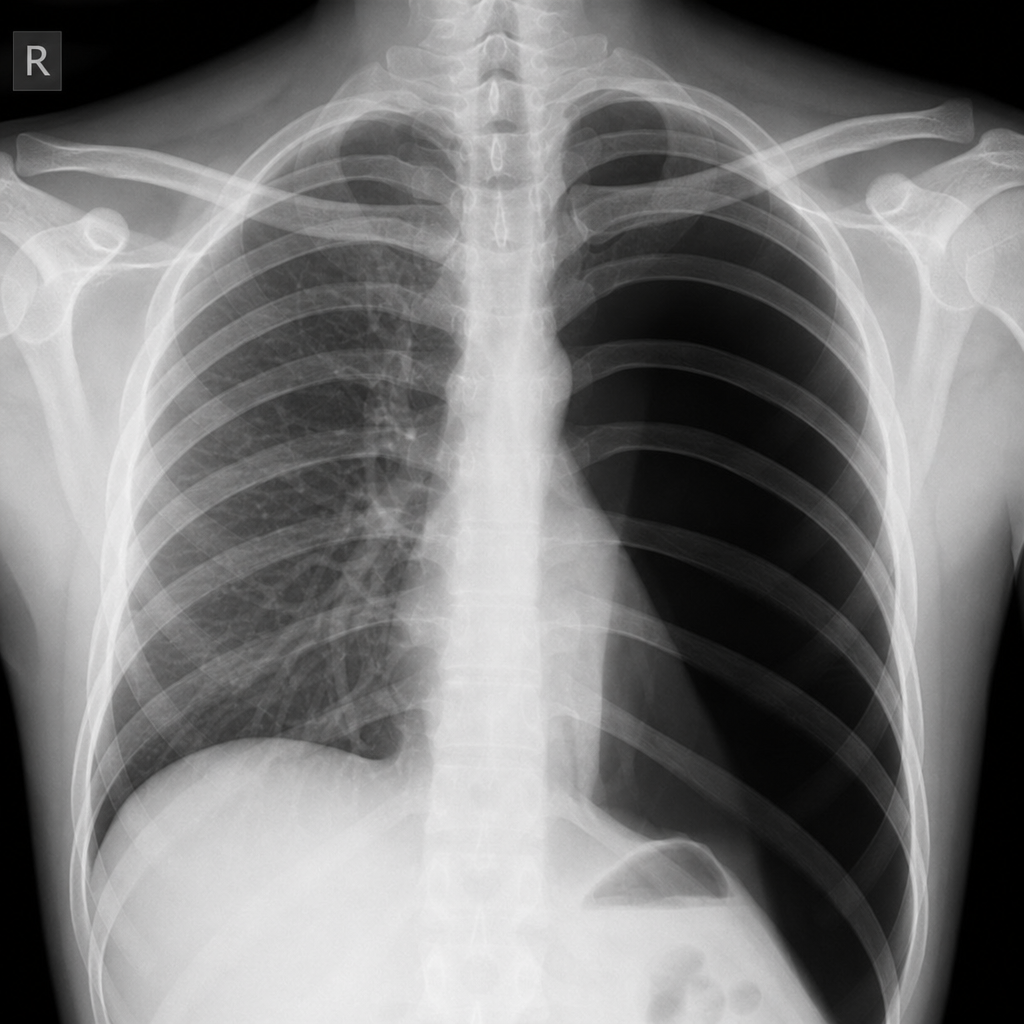
A 25-year-old man presented to the emergency medicine department with acute onset sharp pain and dyspnea. His chest X-ray is provided. What is the diagnosis?
A patient on spirometry shows FEV1/FVC <0.7 and FEV1 >=30% but <50% predicted. What is the patient's diagnosis according to GOLD criteria?
Pleural effusion with very low glucose is typically associated with which of the following conditions?
A 64-year-old man presents with fever, chills, and increasing shortness of breath. The patient appears in acute respiratory distress and complains of pleuritic chest pain. Physical examination shows crackles and decreased breath sounds over both lung fields. The patient exhibits tachypnea with flaring of the nares. The sputum is rusty-yellow and displays numerous neutrophils and erythrocytes. The patient is appropriately treated with antibiotics. Which of the following is the most likely outcome?
A 33-year-old farmer presents with recurrent wheezing and coughing after working in a barn where hay is stored. He has no prior history of asthma and is not taking any medications. Physical examination reveals bibasilar crackles on auscultation, normal heart sounds, JVP of 2 cm above the sternal angle, and no peripheral edema. Laboratory investigations are normal with no increase in eosinophils on the CBC. Chest x-ray reveals patchy lower lobe infiltrates and a normal cardiac silhouette. What is the most likely diagnosis?
A 28-year-old pregnant woman develops sudden onset of dyspnea and tachycardia with no other physical findings. Which of the following is the most likely diagnosis?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app