
Pulmonology — MCQs

On this page
Reactivation of pulmonary tuberculosis always occurs at which location?
Which of the following components is included in the CURB-65 score?
Which of the following is the initial management strategy for chronic obstructive pulmonary disease?
All of the following are characterized by upper lobe fibrosis except?
In pulmonary embolism, what is the primary risk associated with fibrinolytic therapy?
What is the typical sequence of symptoms in pulmonary embolism?
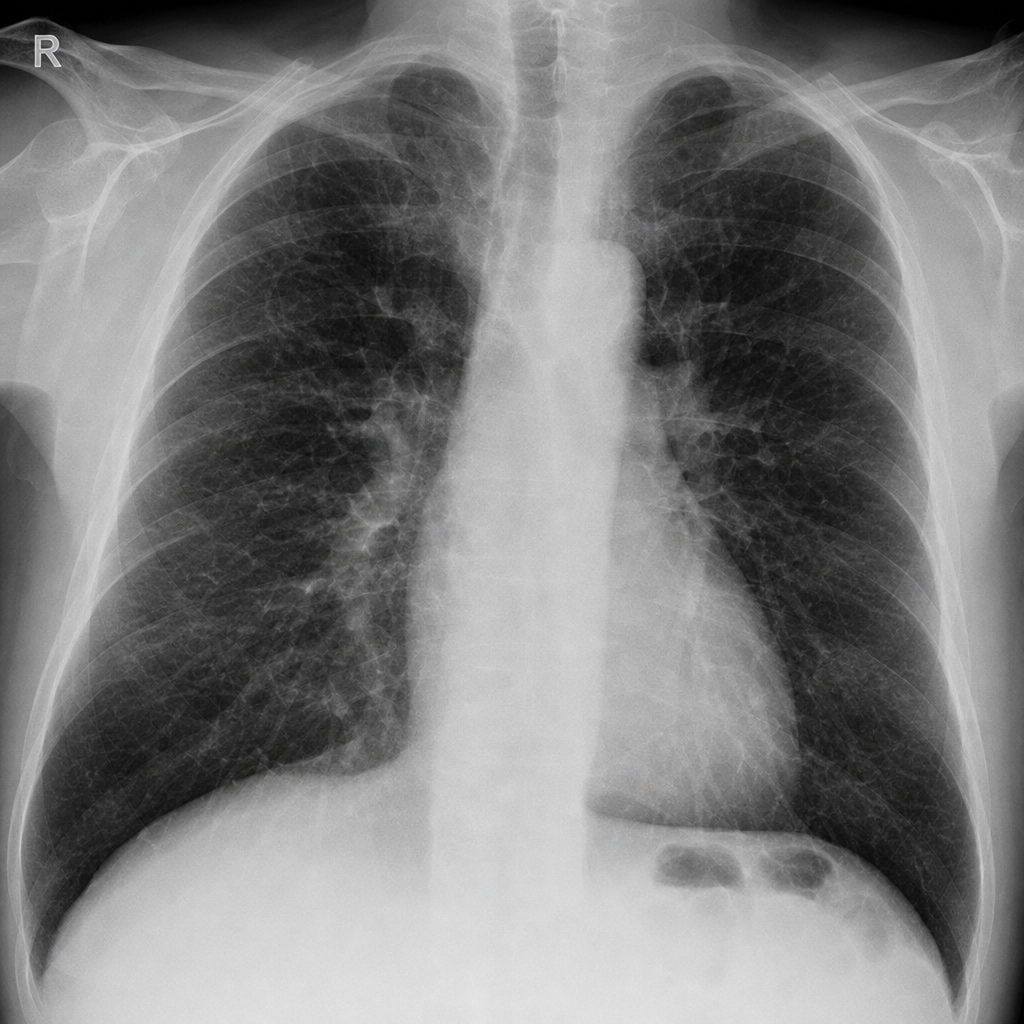
An elderly male, a chronic smoker with 40 pack-years, complains of recurrent difficulty in breathing. A chest X-ray showed abnormalities. Which of the following positions is most comfortable for a patient experiencing difficulty in breathing?
Which of the following conditions may lead to exudative pleural effusions?
A patient presents with left hemiplegia and a history of right deep vein thrombosis. What is the most likely cause of hemoptysis in this patient?
Which of the following conditions can present with an obstructive pattern on pulmonary function tests in an Interstitial Lung Disease (ILD)?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app