
Pulmonology — MCQs

On this page
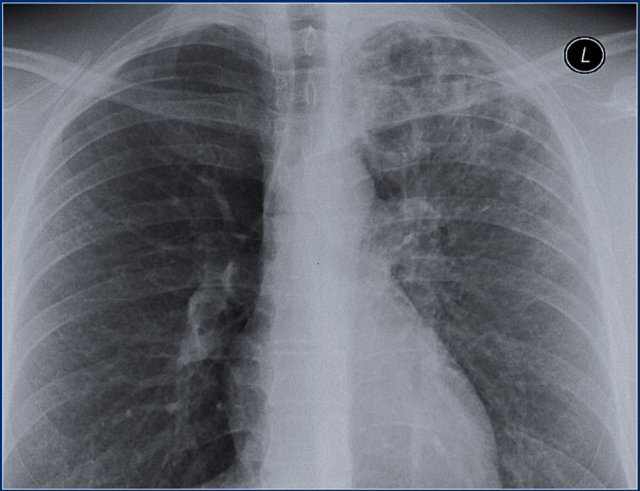
A 70-year-old male smoker presents with cough and sputum production, but is afebrile. Lung examination reveals left-sided crackles, rhonchi, and egophony in the left upper lobe. The patient is being treated for an acute exacerbation of chronic bronchitis, and sputum is negative for AFB. A prior chest X-ray from 5 years ago shows the same left upper lobe findings, unchanged. The current chest X-ray demonstrates left upper lobe fibrotic scarring, volume loss, and calcified granulomas, consistent with chronic stable changes. What is the most likely cause of the observed chest X-ray findings in the left upper lobe?
A 62-year-old man with a 40-pack/year history of smoking presents with increased sputum production and marked shortness of breath. On examination, he is using accessory muscles of respiration, and breath sounds are diminished with expiratory wheezes. Your clinical diagnosis is chronic obstructive pulmonary disease (COPD) exacerbation. For the above patient, select the characteristic arterial pulse finding.
Which of the following is NOT a recognized cause of adult respiratory distress syndrome?
True about pleural effusion?
SIADH is associated with which type of lung malignancy?
Which of the following is NOT associated with pulmonary arterial hypertension?
Type I respiratory failure best relates to which of the following?
A woman presents with a 6-week history of low-grade fever. A chest radiograph shows bihilar adenopathy with clear lung fields. Which of the following investigations would NOT be useful in the differential diagnosis?
A 25-year-old man presents with infertility, a lifelong history of productive cough, recurrent pulmonary infections, chronic abdominal pain, diarrhea, difficulty gaining weight, and diabetes mellitus. His chest x-ray suggests bronchiectasis. What is the most likely diagnosis?
Alpha-1 antitrypsin deficiency presents as which of the following conditions?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app