
Pulmonology — MCQs

On this page
Bronchiectasis is most common in which lobe?
A 27-year-old man presents with new left-sided chest pain and feeling unwell. He describes a 2-day history of cough with some blood-tinged sputum, fever, and chills. His past medical history is negative, and he smokes about 1 pack of cigarettes per day. On physical examination, there is dullness and crackles in the left lower chest. Which of the following is the most likely diagnosis?
Which one of the following distinguishes ARDS (acute respiratory distress syndrome) from cardiogenic pulmonary edema?
A 26-year-old male presents with a history suggestive of tuberculosis and pleural effusion on examination. Which of the following parameters is NOT used for the analysis of pleural fluid in this context?
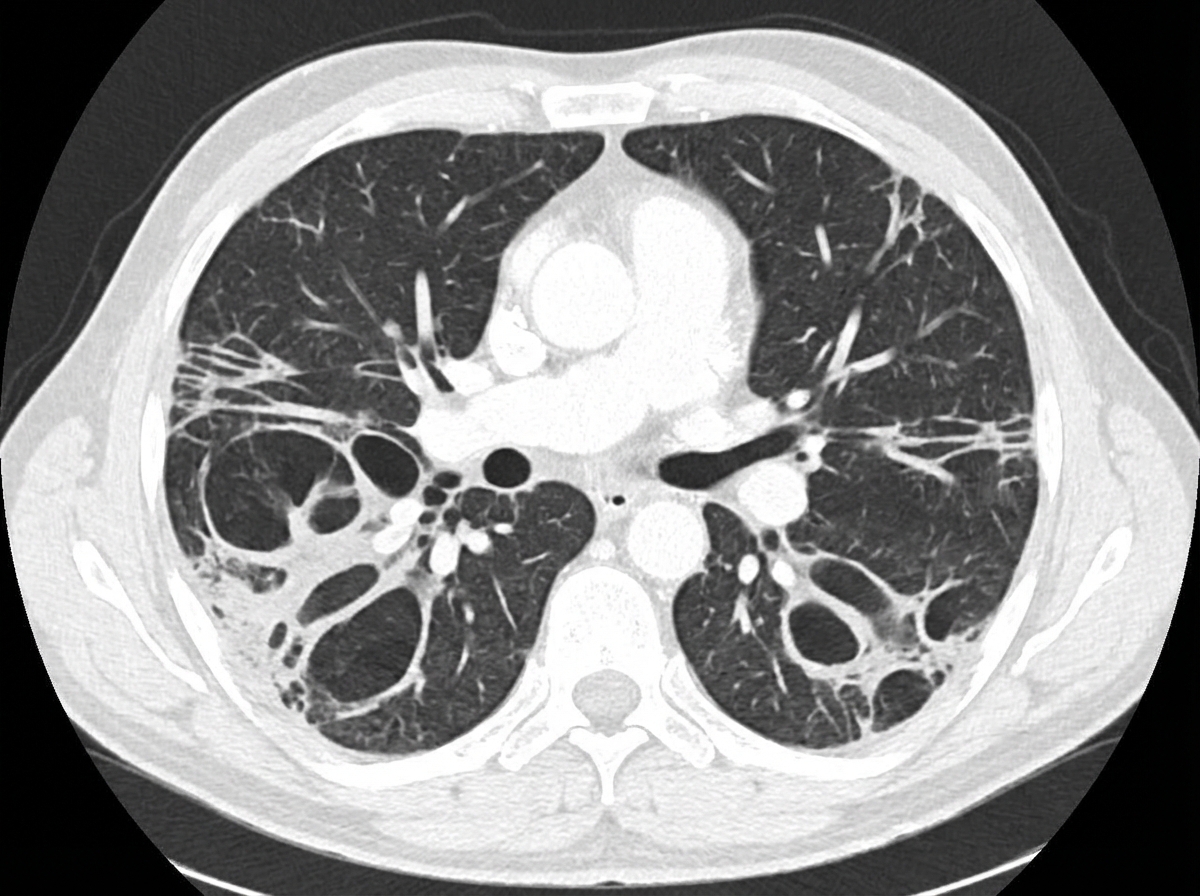
A 55-year-old non-smoker lady presented with on and off haemoptysis and productive cough for 1 year. There was no fever or constitutional symptoms. Physical examination showed clubbing of fingers and coarse crepitations over the lung base. Blood tests were essentially normal and an initial CXR and CT scan were performed. What is the radiological diagnosis?
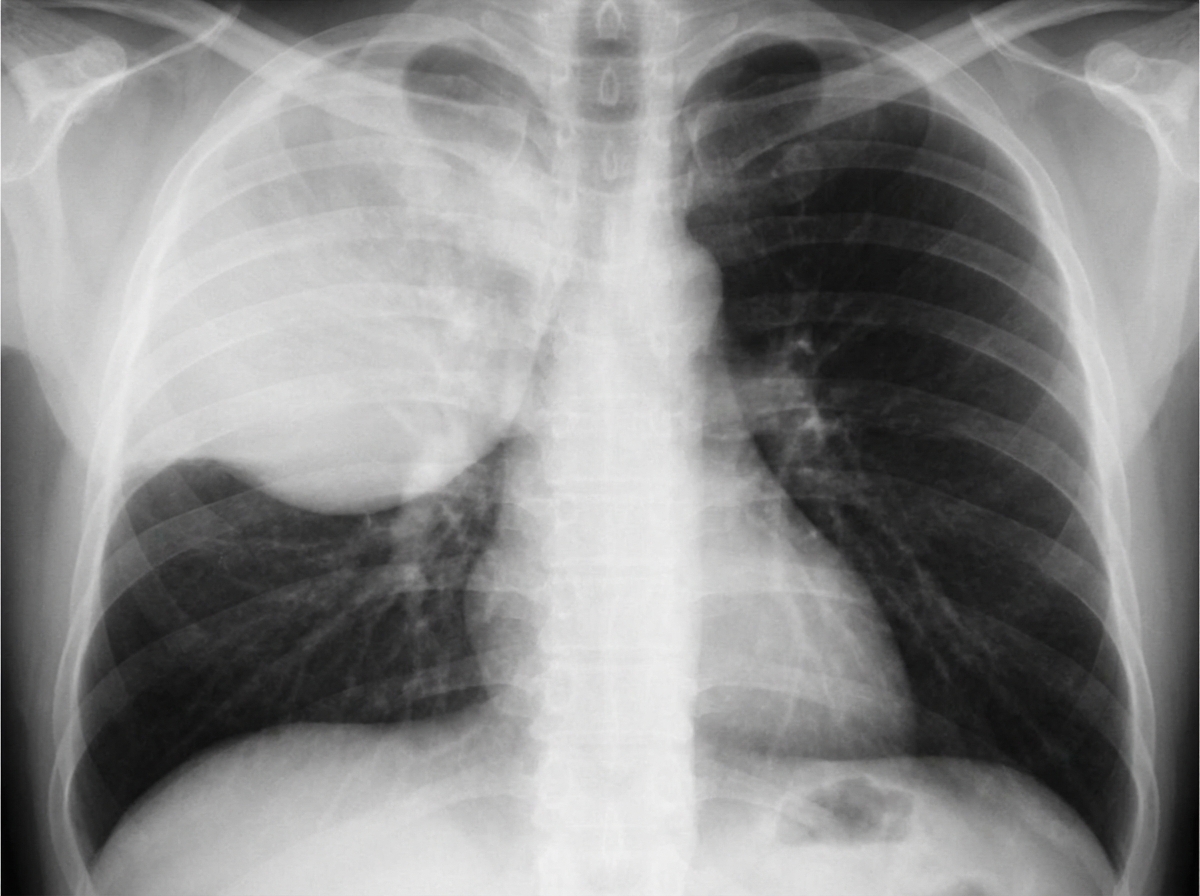
A 34-year-old woman is admitted with a history of fever, chills, and greenish sputum for 10 days. She has a history of alcohol and substance abuse. On physical examination, vital signs are: pulse 113 bpm; temperature 101degF; respirations 25/min; blood pressure 110/78 mm Hg. She appears ill and has crackles with egophony and E to A changes in the right upper lung field. Laboratory data: Hb 12 g/dL; Hct 37%; WBCs 15,000/uL; differential BUN 48 mg/dL; creatinine 1.7 mg/dL. Chest radiographs are shown. What is the most likely diagnosis?
The absence of which of the following signs or symptoms makes a diagnosis of pulmonary embolism unlikely?
Although asthma is a heterogeneous disease, which of the following is most likely to be present in all individuals with asthma?
Which of the following are true about Kartagener's syndrome?
A 50-year-old male presents with dyspnea, dry cough, fatigue, and anorexia. Investigations reveal a raised ESR and a restrictive pattern in pulmonary function tests. HRCT shows honeycombing in subpleural and basal locations. What is the probable diagnosis?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app