
Pulmonology — MCQs

On this page
Which of the following statements is true regarding pulmonary arterial hypertension (PAH)?
A patient presents with massive thromboembolism and hypotension, with a blood pressure of 88/50 mmHg, even after a 1 L fluid bolus. An echocardiogram shows right ventricular hypokinesis. What is the next best step in management?
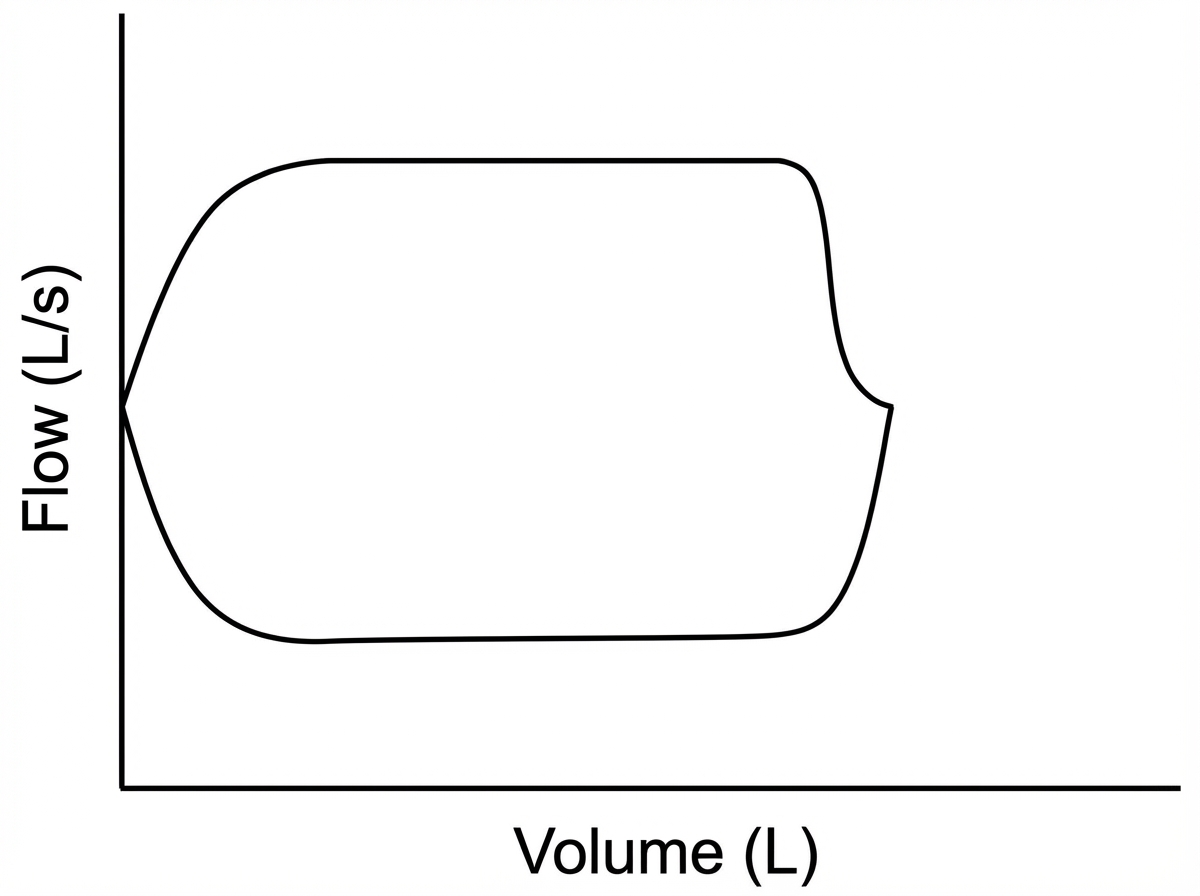
A 65-year-old male presented with progressive dyspnea on exertion for 3 months. His past medical history includes necrotizing pancreatitis and ARDS, for which he was mechanically ventilated. He is a chronic smoker. On examination, low-pitched inspiratory and expiratory wheezes are heard over the mid-chest area. Pulmonary function tests revealed an FEV1 of 78% of predicted and an FEV1/FVC ratio of 60%. A flow-volume curve was also obtained. What is the most likely diagnosis in this case?
A 27-year-old man with a history of chronic sinus and pulmonary infections presents for evaluation. He works as a salesperson and denies specific occupational exposure. He is married and has no children. Family and travel history are noncontributory. Examination reveals crackles in both lower lung zones and extremities show no clubbing. Chest X-ray shows the cardiac apex displaced to the right side of the chest with the gastric bubble also noted on the right. What is the most likely diagnosis?
A 67-year-old woman presents with symptoms of dyspnea. Pulmonary function tests reveal a prominent reduction in the FEV1/FVC ratio. What is the most likely diagnosis?
A patient presents with cough and expectoration. Diagnosis of farmer's lung is suspected. Which statement regarding this condition is true?
Which of the following statements about sarcoidosis is false?
Type I Respiratory failure is seen in which of the following conditions?
All of the following statements are false regarding sarcoidosis, except?
A 24-year-old female graduate student reports increasing shortness of breath with exercise and has recently noticed dyspnea on mild activity. One day before presenting at the office, she experienced sudden loss of consciousness while shopping at a grocery store. On physical examination, vital signs are: pulse 88 bpm; temperature 97.8degF; respirations 18/min; blood pressure 100/70 mm Hg. BMI is 34. ABGs on RA: pH 7.43; PCO2 36 mm Hg; PO2 87 mm Hg. Chest x-rays are shown. What clinical and chest radiographic diagnosis may be commonly associated with this presentation?

Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app