
Pulmonology — MCQs

On this page
Type IV respiratory failure best relates to which of the following?
A 55-year-old man, who has been on bed rest for the past 10 days, complains of breathlessness and chest pain. The chest X-ray is normal. What is the next step in investigation?
Which of the following signs is NOT suggestive of pulmonary embolism?
Smoking is generally not associated as a risk factor with which of the following conditions?
A 60-year-old female presented to the casualty with a fracture of the neck of the femur. She subsequently developed chest pain and breathlessness. What is the most likely diagnosis?
Which of the following findings is NOT typically associated with bronchial breathing?
In bronchiectasis, which of the following findings is NOT typically seen?
All of the following are true about intrinsic asthma, except?
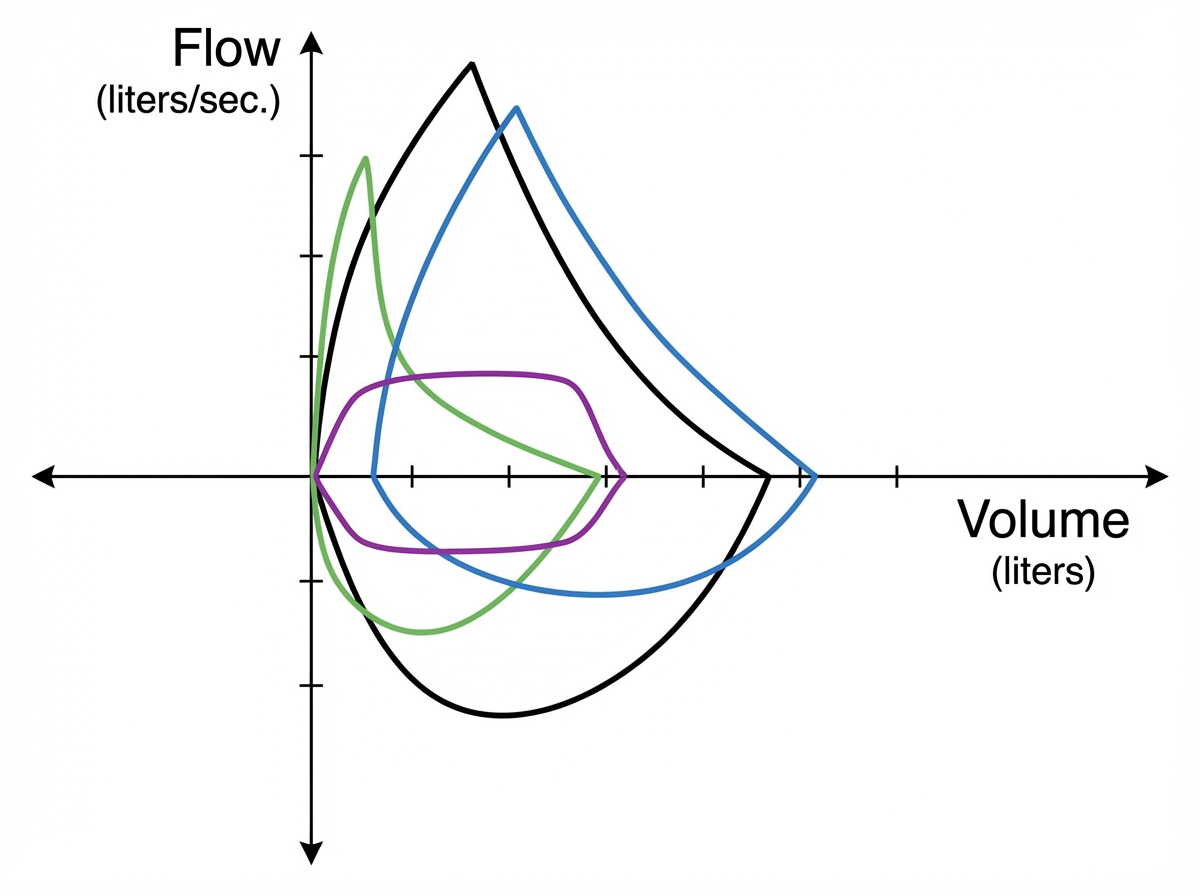
In the pulmonary function test shown in the colour palette, what does the green line represent?
What is a criterion for the diagnosis of acute respiratory distress syndrome?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app