
Pulmonology — MCQs

On this page
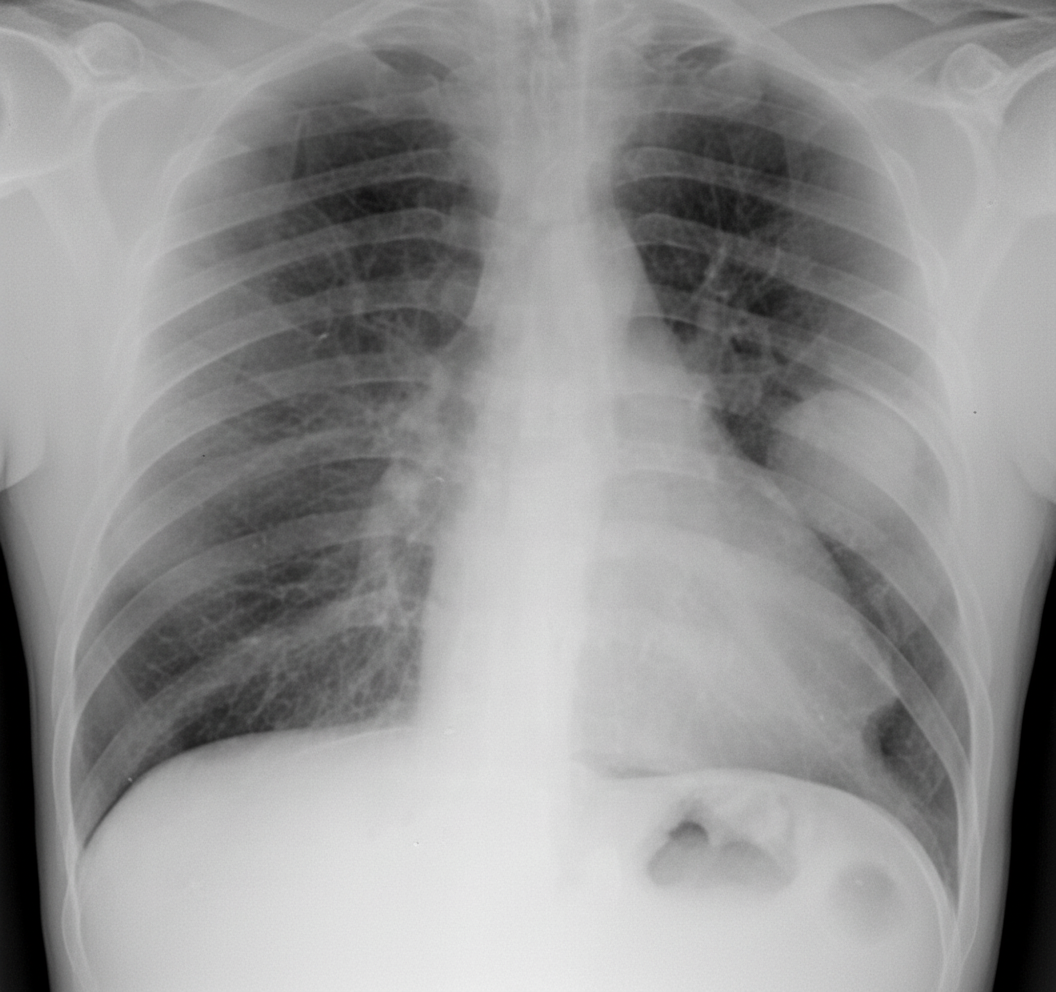
A 60-year-old man with a 30-pack-year smoking history presents with cough and mild hemoptysis. Chest radiography shows a large left perihilar mass. Sputum cytology demonstrates malignant polygonal cells with intercellular bridges and keratin pearls. Which laboratory finding is most characteristic of the paraneoplastic syndrome associated with this tumor?
Which of the following conditions typically presents with an exudative pleural effusion?
Which of the following is NOT a common cause of acute exacerbation of COPD?
What is the most common cause of unilateral diaphragmatic paralysis?
A 55-year-old male presents with a history of hand swelling and shortness of breath. On examination, facial plethora and distended neck veins were noted. Which is the most probable structure involved to cause these symptoms?
A 45-year-old male with a history of alcohol abuse and periodontal disease presents with a spiking fever and chills. Physical examination reveals signs of lung consolidation. A chest x-ray shows a cavity in the right lower lobe with an air/fluid level. Based upon the clinical presentation, which of the following would be the most likely causative organism?
A 47-year-old female with a history of Antiphospholipid antibody syndrome, who has been non-compliant with warfarin, presents with deep vein thrombosis and dyspnea. She is hypotensive and tachypneic. CT of the chest shows a saddle embolus. She does not respond to heparin and fluids. Echocardiogram shows RV hypokinesis. Which of the following is the appropriate management?
Which of the following is the most potent stimulus for the development of cor pulmonale in patients with chronic obstructive pulmonary disease?
Which of the following is NOT true about sarcoidosis?
Serum angiotensin-converting enzyme may be raised in all of the following, except?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app