
Pulmonology — MCQs

On this page
Which of the following correlates well with the severe type of bronchial asthma exacerbation?
A 23-year-old man is experiencing a flare of his asthma. He is using his salbutamol inhaler more frequently than usual and despite increasing his inhaled steroids he is still short of breath. Previously, his asthma was considered mild with no severe exacerbations requiring oral steroids or hospitalization. With the current flare, he is experiencing recurrent episodes of bronchial obstruction, fever, malaise, and expectoration of brownish mucous plugs. On examination, there is bilateral wheezing. The heart, abdomen, neurologic, and skin exams are normal. A CXR reveals upper lobe pulmonary infiltrates; the eosinophil count is 3000/mL, and serum precipitating antibodies to Aspergillus are positive. Which of the following is the most likely diagnosis?
Following pelvic gynecologic surgery, a 34-year-old woman becomes dyspneic, her peripheral arterial O2 saturation falls from 94% to 81%, and her measured PaO2 is 52 on a 100% non-rebreather mask. She is hemodynamically stable. A CT angiogram is consistent with a right lower lobe pulmonary embolus. Which of the following is the next step in her management?
Which of the following is used for the management of pneumomediastinum?
What is the most common cause of diffuse bronchiectasis?
A 60-year-old chronic smoker presents with weight loss, cough, and hemoptysis. A chest radiograph revealed a specific appearance. The patient subsequently developed gradually progressive left upper limb pain, paresthesia, and weakness. He also developed left-sided Horner's syndrome. What is the most likely diagnosis?
What is true about Bronchial Asthma?
A 16-year-old asthmatic uses a salbutamol inhaler twice a week on average and frequently wakes up coughing. She is compliant with her treatment regimen and has good inhaler technique. Which of the following would be the most appropriate next step in managing her asthma?
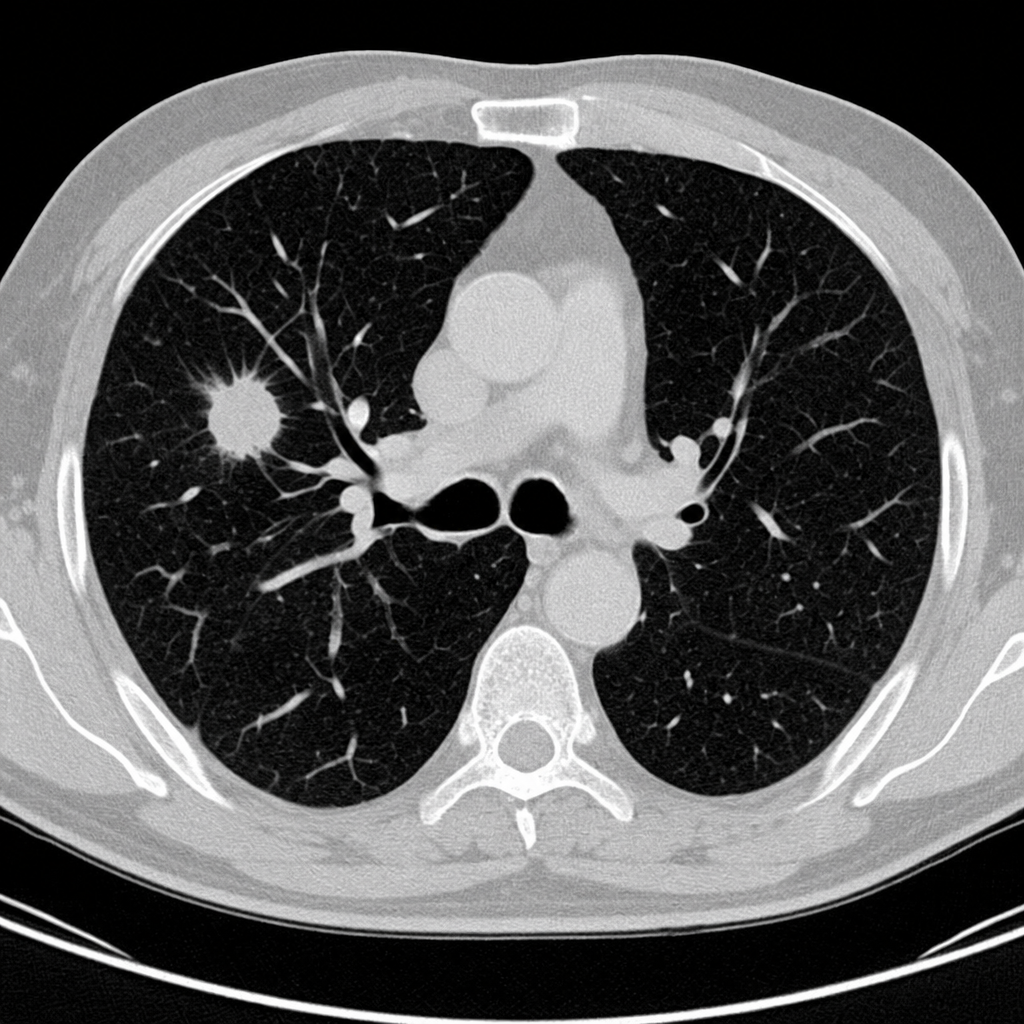
A 57-year-old recently retired demolitions worker complains of increasing shortness of breath. The patient was a chronic heavy cigarette smoker throughout his adult life but quit about a year before presentation. A chest CT was performed and reveals a 2.8 cm spiculated nodule in the right upper lobe without a bronchus sign, with a high pretest probability of malignancy. Which of the following steps is not appropriate in the evaluation of this patient?
A 65-year-old miner presents with a two-month history of 7 kg weight loss, cough, and blood-streaked sputum. He had a history of pulmonary tuberculosis 10 years ago. He also reports drooping of his left eyelid for one month. Physical examination reveals left-sided ptosis and pupillary miosis. Chest X-ray shows a round opacification in the left upper apical lobe. What is the most probable diagnosis?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app