
Pulmonology — MCQs

On this page
Which of the following is false regarding the CURB-65 criteria used to assess pneumonia severity?
What is the major risk factor for the development of a lung abscess?
A 25-year-old man presents with a progressive illness of several days' duration characterized by nonproductive cough, fever, and malaise. A lateral view chest radiograph reveals platelike atelectasis. Elevated titers of cold agglutinins are detected. Which of the following is the most likely type of pneumonia in this patient?
Hemoptysis is commonly seen in:
What is true about sarcoidosis?
Extensive pleural thickening, especially involving the diaphragmatic pleura, is a classical feature of which condition?
What is the initial management for a spontaneous pneumothorax?
All of the following conditions may predispose to pulmonary embolism except?
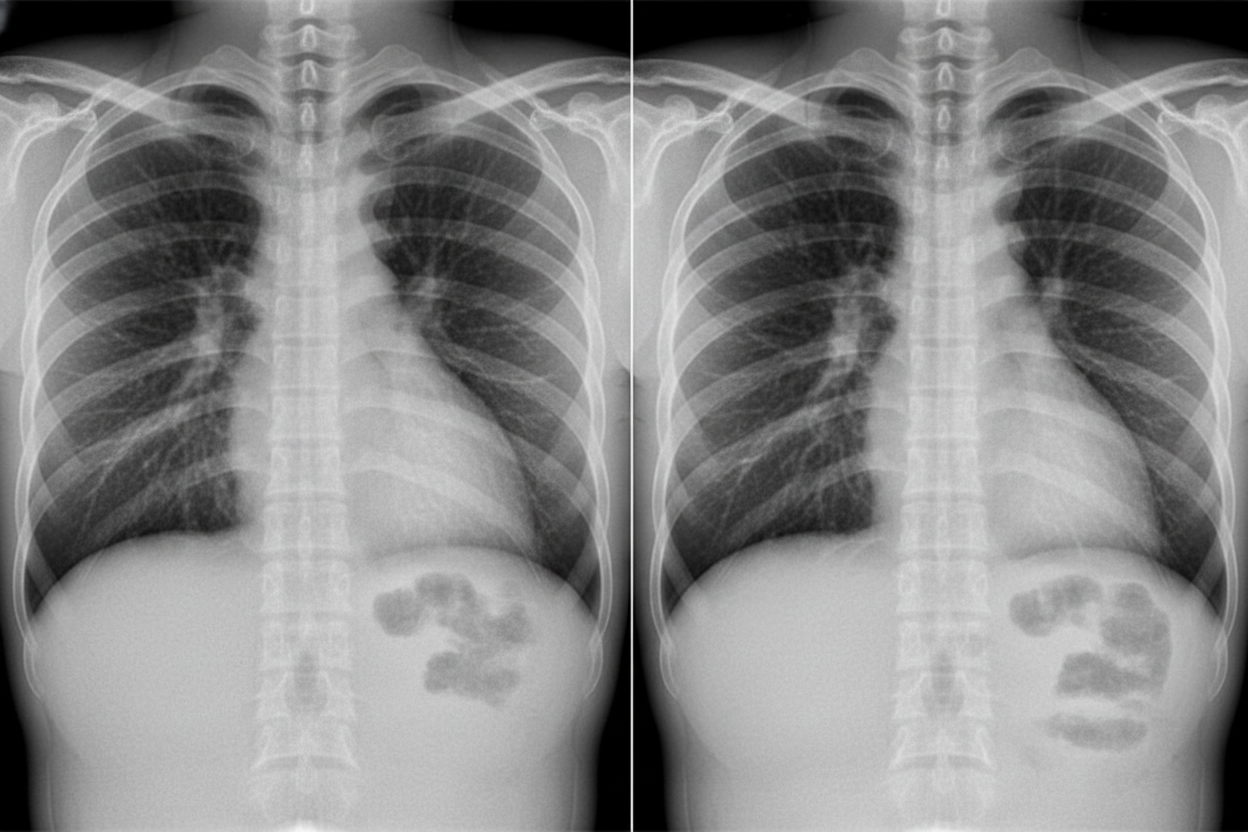
A patient presents with acute onset high-grade fever, chills, productive cough with rusty-colored sputum, and pleuritic chest pain. The chest X-ray is shown below. What is the most likely diagnosis?
Exudative pleural effusion is seen in:
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app