
Pulmonology — MCQs

On this page
Bronchoalveolar lavage is beneficial in the evaluation of which condition?
A chronic smoker presents with complaints of haemoptysis. Chest X-ray appears to be normal. What is the next best investigation?
A non-smoker patient presents with a cough of more than 3 months duration and a normal chest X-ray. All of the following are potential causes of chronic cough EXCEPT:
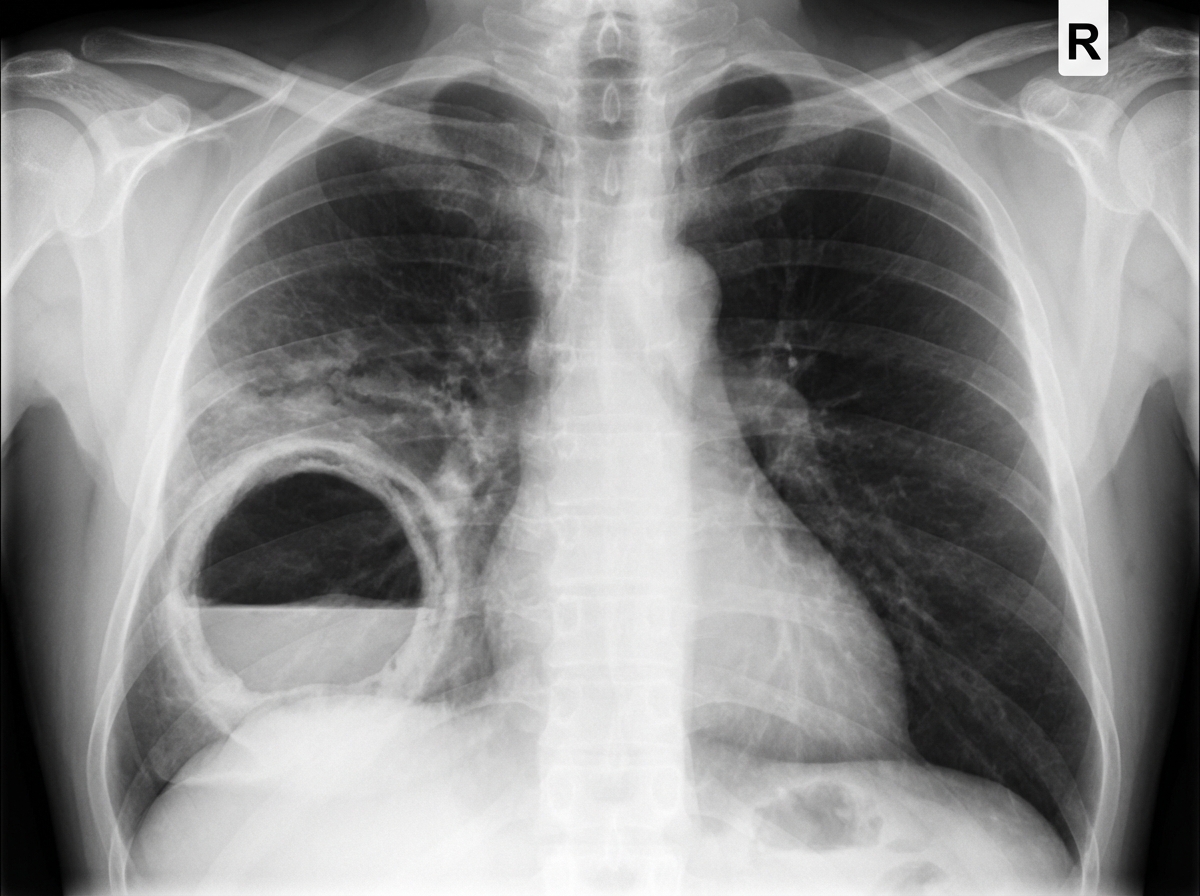
A 40-year-old man with a history of substance abuse and HIV infection presents with fever, weight loss, production of foul-smelling sputum, and shortness of breath for 2 weeks. Physical examination reveals tachypnea and clubbing of his digits. Lung auscultation demonstrates diffuse rhonchi and an area of egophony with whispering pectoriloquy in the right posterior chest. Arterial blood gases show a PaO2 of 59 mm Hg on room air. A chest X-ray is available. What is the most likely diagnosis?
Proximal bronchiectasis and segmental collapse in a patient with chronic persistent asthma should raise suspicion for which of the following conditions?
Which of the following is the investigation of choice for interstitial lung disease?
In a patient with pulmonary embolism, right ventricle hypokinesia, and decreased output, which drug therapy is most helpful?
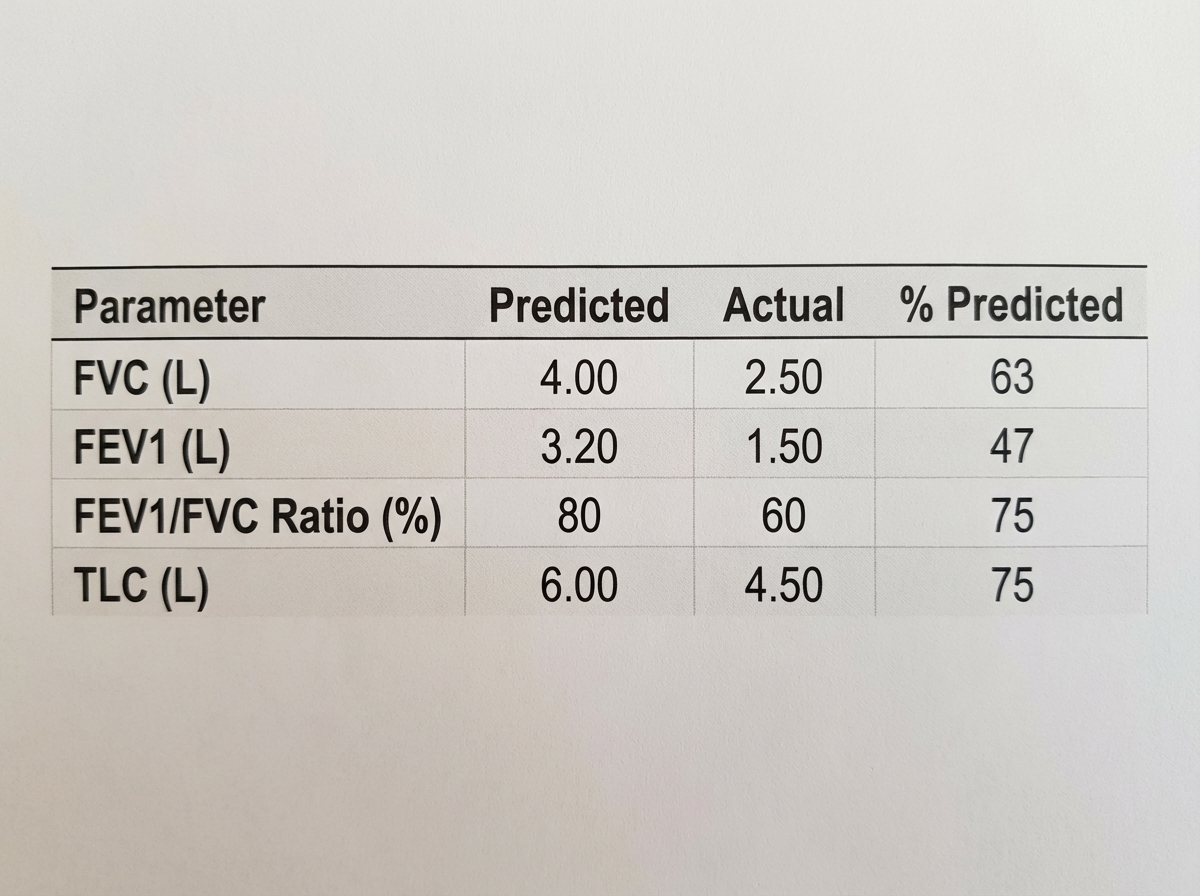
A 64-year-old woman presents with complaints of dyspnea and orthopnea. She is a lifelong non-smoker. Her pulmonary function testing is as follows. What is the most probable diagnosis?
A 23-year-old man is experiencing a flare of his asthma. He is using his salbutamol inhaler more frequently than usual and despite increasing his inhaled steroids, he is still short of breath. Previously, his asthma was considered mild with no severe exacerbations requiring oral steroids or hospitalization. With his flare, he has recurrent episodes of bronchial obstruction, fever, malaise, and expectoration of brownish mucous plugs. On examination, there is bilateral wheezing. The heart, abdomen, neurologic, and skin exams are normal. CXR reveals upper lobe pulmonary infiltrates; the eosinophil count is 3000/mL, and serum precipitating antibodies to Aspergillus are positive. Which of the following is the most likely diagnosis?
What is the most common symptom of Pulmonary embolism?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app