
Pulmonology — MCQs

On this page
Which of the following findings is NOT typically seen in lung function tests for emphysema?
Which of the following signs will not be present in pleural effusion?
Which subtype of interstitial lung disease is seen in patients with Sjogren syndrome?
In a case of pleural effusion caused by pneumococcal pneumonia, chest tube insertion is indicated in all of the following pleural fluid findings, EXCEPT:
Which of the following statements regarding sarcoidosis is incorrect?
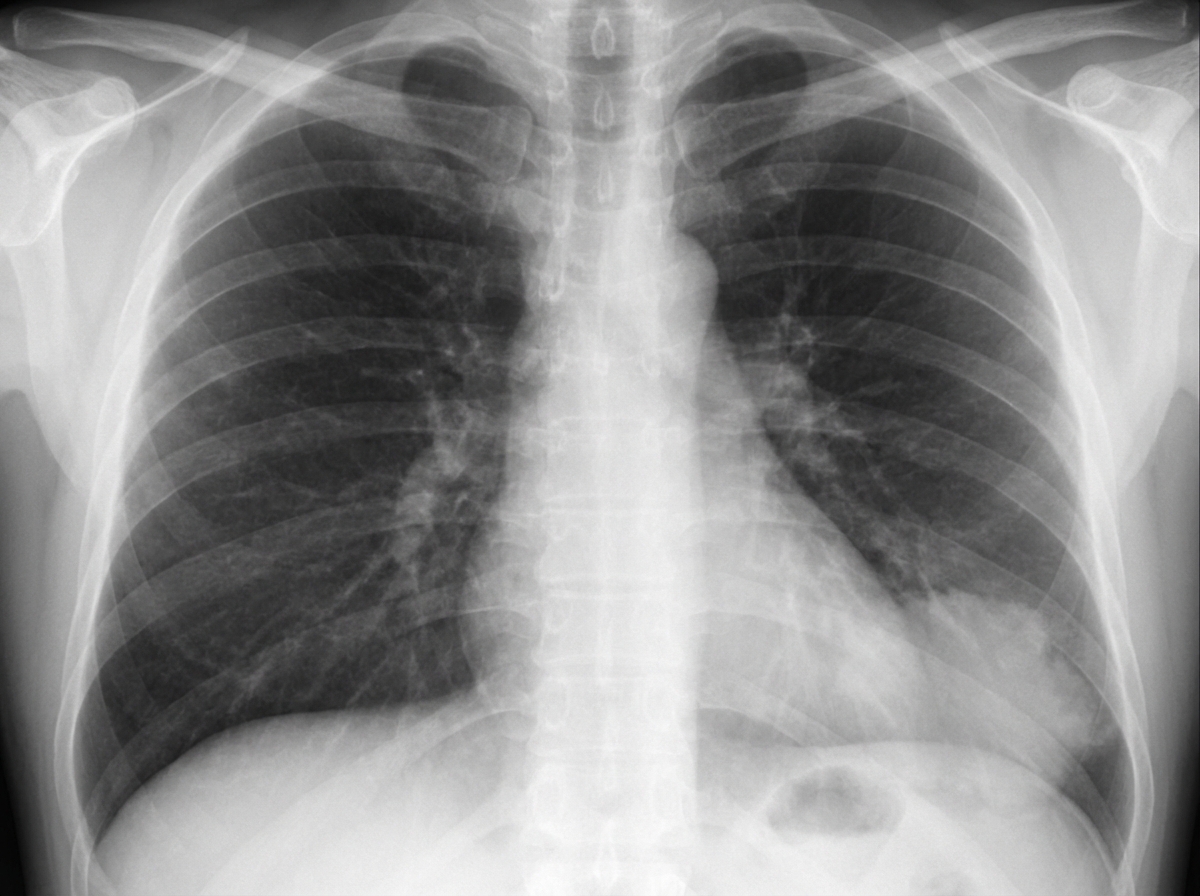
A 29-year-old woman presents with a history of recurrent respiratory tract infections. She has no significant travel history and denies any history of foreign body aspiration. On examination, coarse crackles are noted in the left lower lung zone. A chest X-ray reveals findings suggestive of a possible abnormality. Based on the history and chest X-ray findings, what is the most appropriate next diagnostic step?
A 61-year-old male presents with increasing shortness of breath. A chest x-ray reveals a diffuse pulmonary infiltrate, and a transbronchial biopsy reveals fibrosis of the walls of the alveoli, many of which contain sheets of desquamated cells. Which of the following would be the best therapy for this patient?
Which of the following is NOT a feature of allergic bronchopulmonary aspergillosis (ABPA)?
Which of the following is not a feature of bronchiectasis?
Pneumothorax is not a usual occurrence with which of the following conditions?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app