
Pulmonology — MCQs

On this page
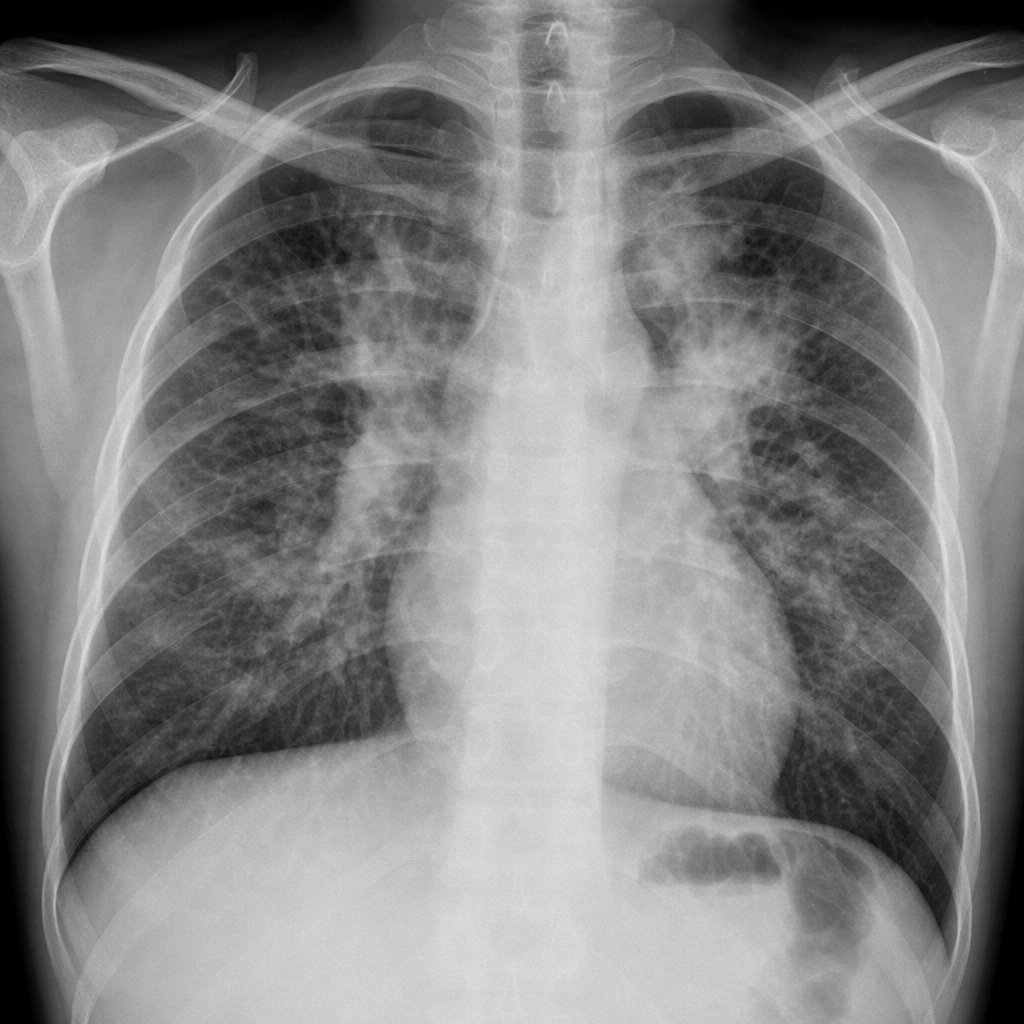
A 34-year-old black female presents with symptoms of cough, dyspnea, and lymphadenopathy. Physical examination reveals hepatomegaly but no palpable peripheral lymph nodes. A chest radiograph was obtained. How should the diagnosis be pursued?
Which of the following statements is NOT true regarding a hydatid cyst of the lung?
Lymphangioleiomyomatosis is characterized by all of the following features except:
A 30-year-old male presents with recurrent hemoptysis. X-ray shows no abnormality. What is the next investigation?
A 30-year-old African-American woman presents with bilateral hilar lymphadenopathy and reticular densities in both lung fields. Which of the following is a defining characteristic of the disorder suggested by these findings?
Pseudochylous pleural effusion is characteristically seen in which of the following conditions?
Which of the following is a clinical feature of pneumonia?
A 25-year-old male with a long history of severe asthma presents to the emergency room with shortness of breath. He has previously required hospital admission and was once intubated for asthma. Which of the following findings on physical exam would indicate a benign course?
A patient with a known case of COPD presents with an acute exacerbation and is managed in the ICU. Which of the following statements is NOT true regarding its management?
A 53-year-old male smoker with progressive shortness of breath, who has received multiple courses of antibiotics for presumed bronchitis, presents with diffuse rhonchi and crackles on lung examination. Arterial blood gases show a PaO2 of 68 mm Hg with mild compensated respiratory alkalosis. Sputum for AFB is negative. Associated with this diagnosis is:
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app