
Pulmonology — MCQs

On this page
What is the drug of choice for diffuse panbronchiolitis?
Which of the following conditions may lead to exudative pleural effusion?
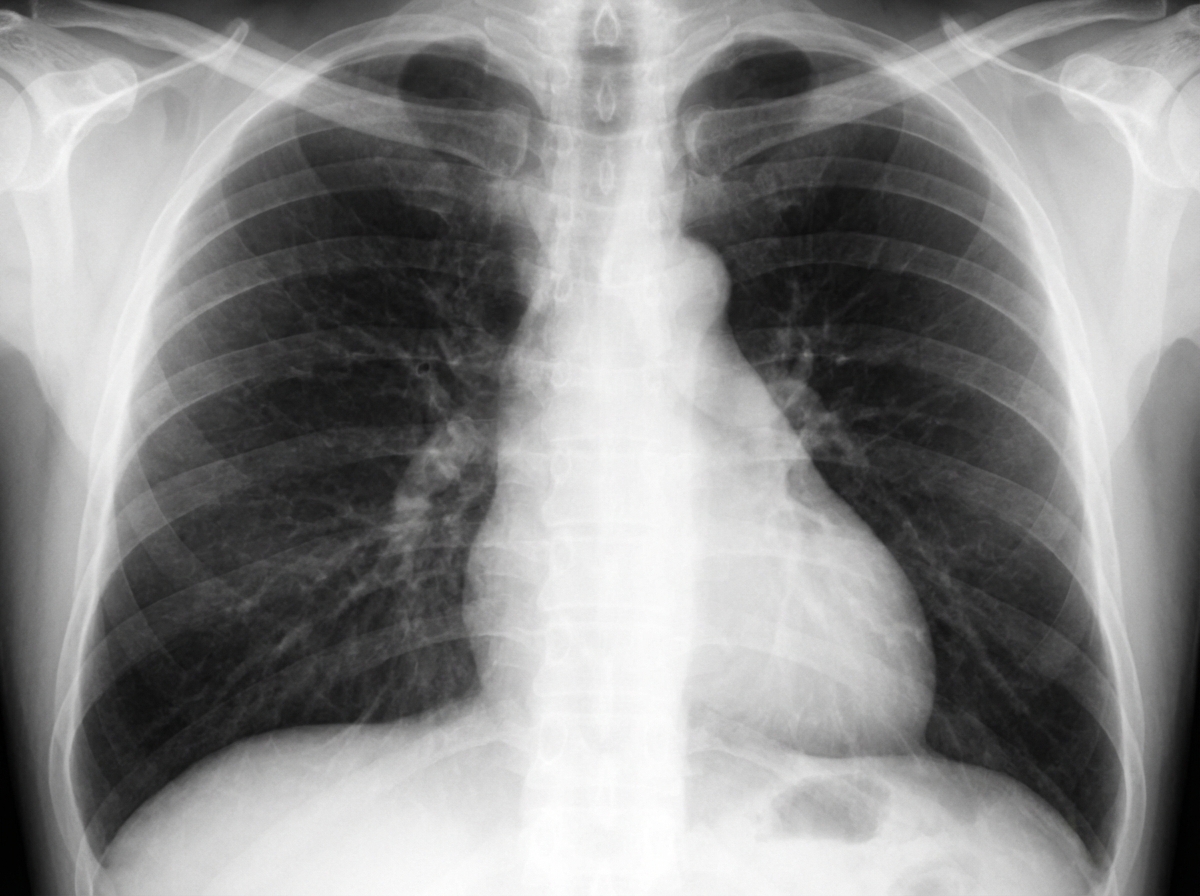
A 41-year-old male schoolteacher, a nonsmoker, presents with lightheadedness, shortness of breath, "lack of stamina," and chest pain. On physical examination, vital signs are normal. The patient is overweight with a BMI of 33. Cardiovascular examination reveals a left parasternal heave, a harsh grade 3/6 systolic flow murmur, and a loud P2 sound. Chest radiographs are shown. What is the most likely diagnosis?
What is the recommended treatment for cough variant asthma?
Hospital-acquired pneumonia is defined as an infection occurring how many days after hospital admission?
What is the treatment most likely to benefit a patient with massive pulmonary embolism presenting in shock?
Which of the following is NOT seen in a Pancoast tumor?
Hypoxemia occurring after pulmonary thromboembolism is a result of which of the following?
What is the effect of rheumatoid arthritis on the lung?
All of the following are seen in massive pulmonary embolism except:
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app