
Pulmonology — MCQs

On this page
Which of the following statements regarding hypersensitivity pneumonitis is FALSE?
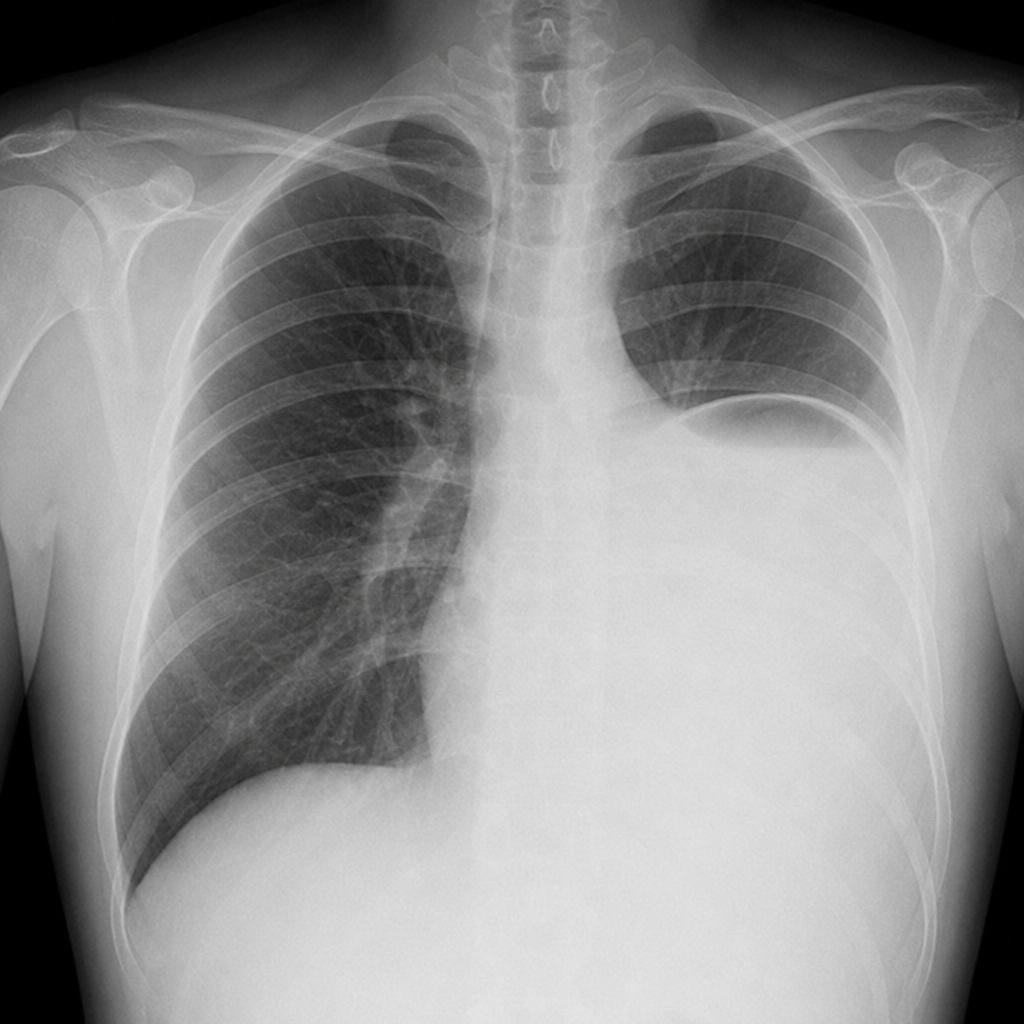
A 37-year-old truck driver presents with recent onset of shortness of breath, aggravated by bending over, lying down, and exertion. Physical examination reveals normal vital signs, decreased air movement at the left base with an area of dullness posteriorly on lung auscultation, and a soft abdomen without palpable organomegaly. A chest X-ray is shown. Which diagnostic test would best confirm the diagnosis?
A patient presents with sudden respiratory distress. On examination, bilateral basal crepitations are noted, suggestive of pulmonary edema with normal alveolar-wedge pressure. What is the likely cause?
Which of the following classes of drugs is a precipitant of acute asthma?
A 35-year-old man presents with shortness of breath and no history of lung or heart disease. He smokes half a pack a day and has for 10 years. Examination reveals a JVP of 2 cm, normal heart sounds, and clear lungs. Chest X-ray shows hyperinflation and increased lucency of the lung fields. A chest CT reveals bullae and emphysematous changes. Pulmonary function tests show an FEV1/FVC ratio of less than 70%. His family history is significant for other affected individuals. What is the most likely diagnosis?
Which of the following findings is true in Acute Respiratory Distress Syndrome (ARDS)?
Which of the following is the most common abnormality in ECG manifestation of pulmonary embolism?
All of the following are associated with pulmonary eosinophilic pneumonia, except?
A 48-year-old alcoholic man presents with a 6-day history of productive cough and fever. The temperature is 38.7°C (103°F), respirations are 32 per minute, and blood pressure is 126/86 mm Hg. The patient's cough worsens, and he begins expectorating large amounts of foul-smelling sputum. A chest X-ray shows a right upper and middle lobe infiltrate. A CBC demonstrates leukocytosis (WBC = 38,000/mL), with 80% slightly immature neutrophils and toxic granulation. Laboratory studies reveal elevated leukocyte alkaline phosphatase. Which of the following best describes this patient's hematologic condition?
A 31-year-old man with severe kyphoscoliosis due to cerebral palsy presents with worsening shortness of breath on exertion. He denies chest discomfort, fever, chills, cough, or sputum production. Examination reveals severe scoliosis to the left with decreased air entry on that side. His right lung is clear, JVP is at 3 cm, and heart sounds are normal. Which of the following is the most likely abnormality to be seen on the pulmonary function tests?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app