
Pulmonology — MCQs

On this page
Bilateral symmetrical hilar lymphadenopathy is seen in:
What is the most common cause of lung abscess?
A 45-year-old smoker presents with a 3-week history of productive cough and one episode of coughing up the pictured blood-streaked sputum (not a gelatinous plug). He has no history of asthma or cystic fibrosis. On examination, there is no subcutaneous emphysema, no Horner syndrome, and no wasting of the intrinsic hand muscles. What is the most likely finding accounting for this presentation?

All of the following are features of acute severe asthma EXCEPT?
A 63-year-old man is presenting with facial swelling. What condition is the most likely cause of these findings?
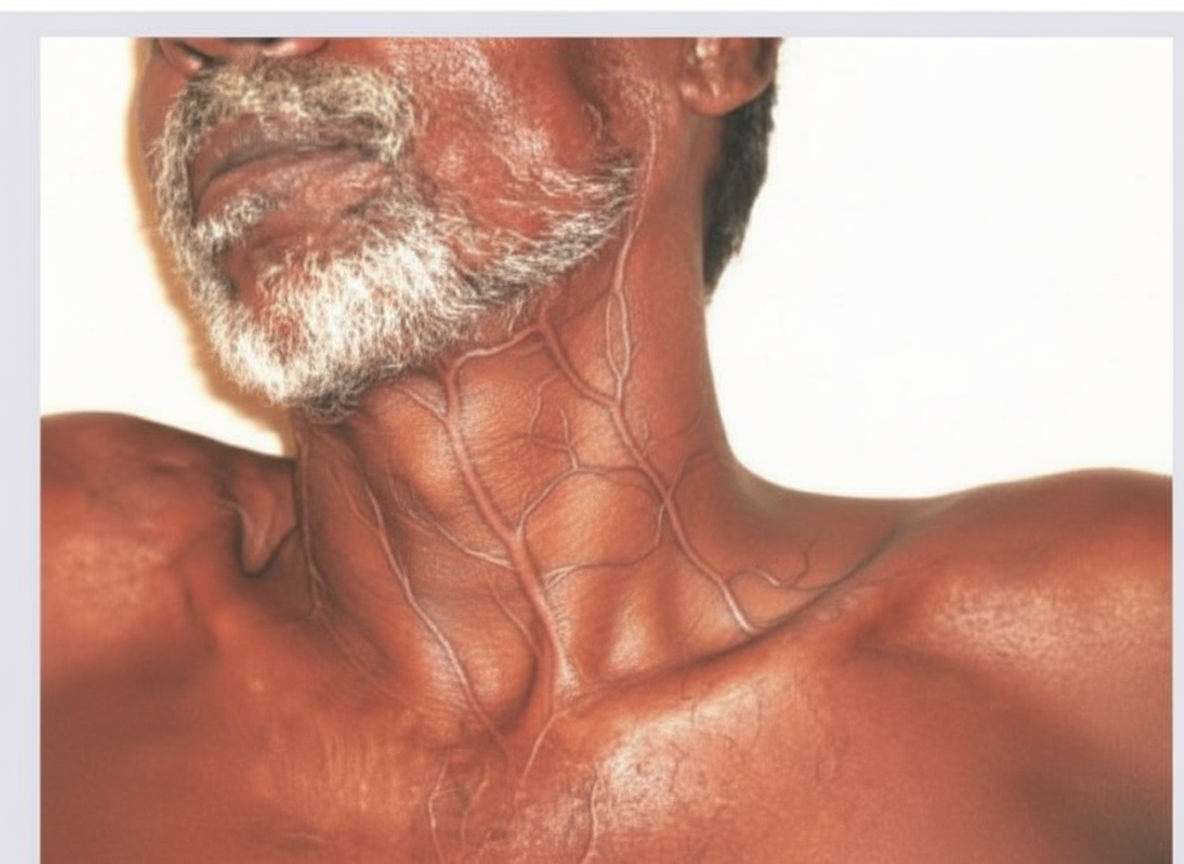
A 54-year-old construction worker has smoked two packs of cigarettes daily for the past 25 years. He notes swelling in his upper extremity and face, along with dilated veins in this region. A computerized tomography (CT) scan and venogram of the neck are performed. What is the most likely cause of the obstruction?
Which of the following is NOT a component of Lofgren syndrome?
Acute severe lung injury is characterized by:
A truck driver presents with a one-month history of chronic cough and fever. Chest X-ray reveals bilateral reticulonodular infiltrates in the mid and lower lung zones. What is the most likely diagnosis?
A 50-year-old male with a known case of emphysema presents with a two-week history of shortness of breath. A chest X-ray reveals a 3 cm pneumothorax on the right side. What is the appropriate management approach for this patient?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app