
Pulmonology — MCQs

On this page
A stony dull note on percussion is characteristic of which of the following conditions?
A 53-year-old man, a smoker for 35 years at a 2-pack-a-day rate, presents with a persistent cough and dyspnea. A chest X-ray reveals an increased anterior-posterior diameter, flattened diaphragms, and air trapping, ruling out malignancy. The patient is informed that his condition is irreversible and that smoking cessation is crucial to halt disease progression. At the molecular level, this disease is caused by which one of the following?
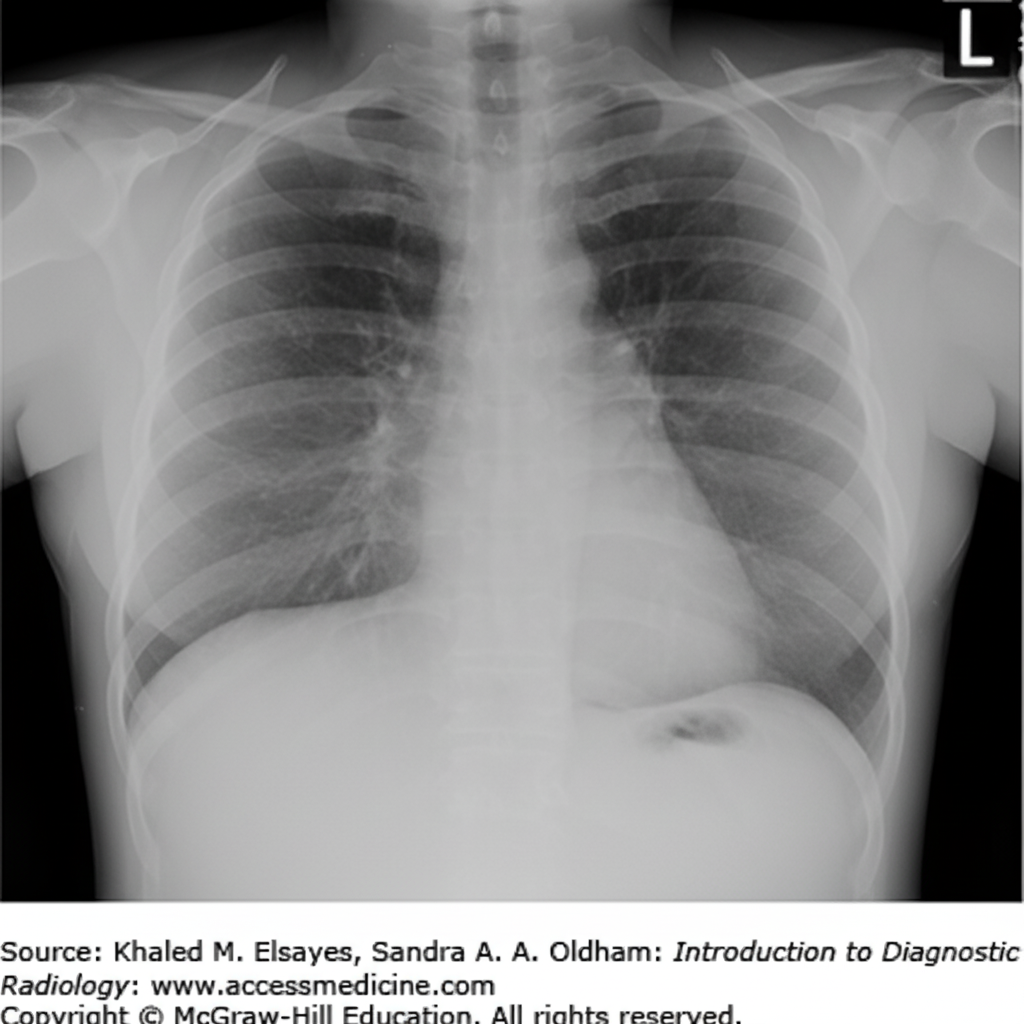
A 41-year-old man presents with severe shortness of breath. He reports a 25-lb weight loss over the last 2 months and occasional vomiting after meals. His vital signs are: pulse 110 bpm, temperature 98 F, respirations 24/min, and blood pressure 110/70 mm Hg. Physical examination reveals dullness to percussion on the left posterior chest with decreased breath sounds. Egophony is heard over the left upper lung field posteriorly. A PPD test is 15 mm. A chest X-ray is shown. What is the most likely diagnosis?
A 60-year-old man is suspected of having endobronchial carcinoma. What is the best investigation?
What is a genetic risk factor for COPD?
A 54-year-old smoker presents with severe hemoptysis, weight loss, and oligoarthritis. Serial skiagrams show fleeting opacities. What is the diagnosis?
A 75-year-old man with no past medical history presents with increasing shortness of breath over 6 months. He previously worked at a shipyard with significant exposure to asbestos. He has a large right-sided pleural effusion. Pleural aspiration reveals an exudate, but cytopathological examination identifies no malignant cells. CT scanning reveals circumferential pleural thickening but no other abnormalities. Which test is most likely to yield a diagnosis?
Bilateral pleural effusion may occur in all of the following conditions except?
A 61-year-old man presents with a persistent, non-productive cough for 1 month. He has no other symptoms. He has been smoking approximately 20 bidis per day for the last 25 years. Physical examination is normal. What is the appropriate line of management?
A 26-year-old African-American woman presents with bilateral hilar adenopathy. Radiography reveals multiple reticular densities in both lung fields. A bronchoscopic biopsy shows granulomatous inflammation with multiple giant cells but no evidence of caseous necrosis. What is the most likely diagnosis?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app