
Pulmonology — MCQs

On this page
A 45-year-old coal mine worker presents with cutaneous nodules, joint pain, and occasional cough with dyspnea. His chest radiograph shows multiple small (1-4 cm) nodules in bilateral lung fields. Some of the nodules show cavitation and specks of calcification. What is the most likely diagnosis?
All of the following interventions are demonstrated to affect the natural history of patients with COPD, except?
Type 2 Respiratory Failure is seen in which of the following conditions?
Loeffler's syndrome is characterized by:
Bilateral exudative pleural effusion is seen in which of the following conditions?
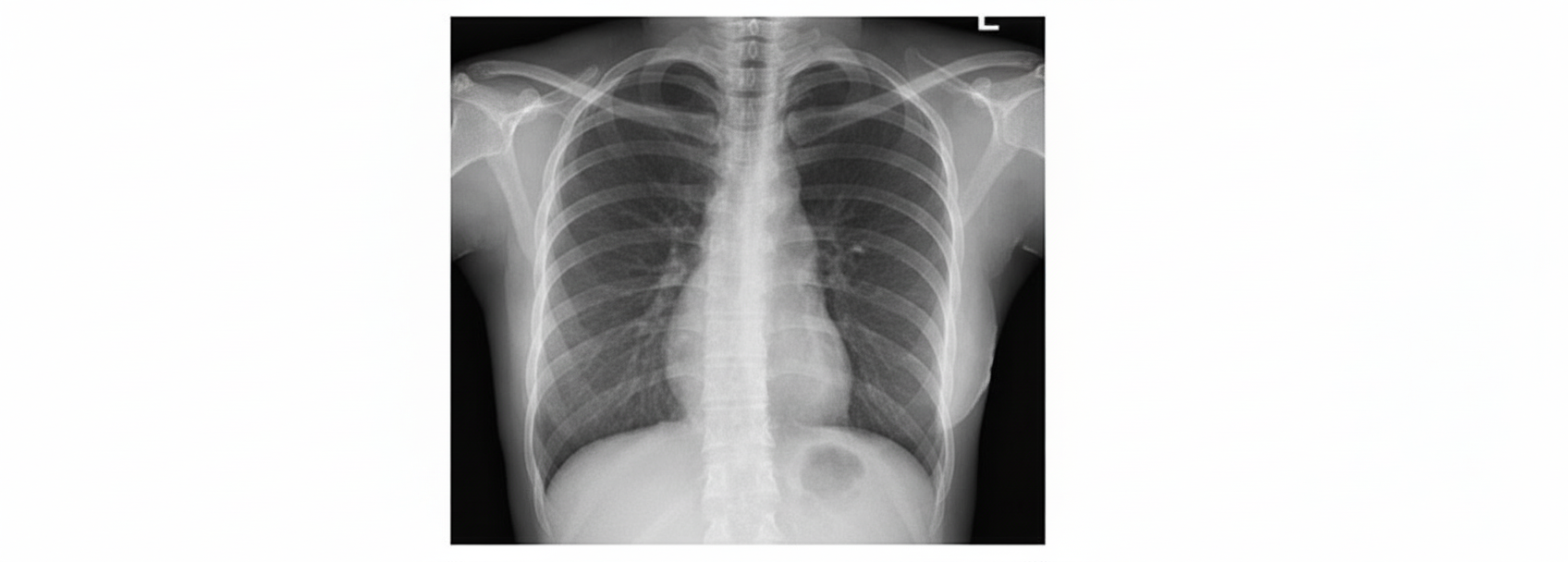
A 32-year-old female presents to the medicine outpatient department with a dry cough for the last few weeks. She complains of difficulty in breathing on exertion and in resting condition as well. On examination, she had erythema nodosum on lower limbs along with painful arthritis. Bilateral hilar lymphadenopathy was noted. Laboratory investigations showed raised levels of Angiotensin-converting enzymes (ACE). Her chest radiograph is shown below. What is the probable diagnosis in this case?
All the following statements about Emphysema are true except?
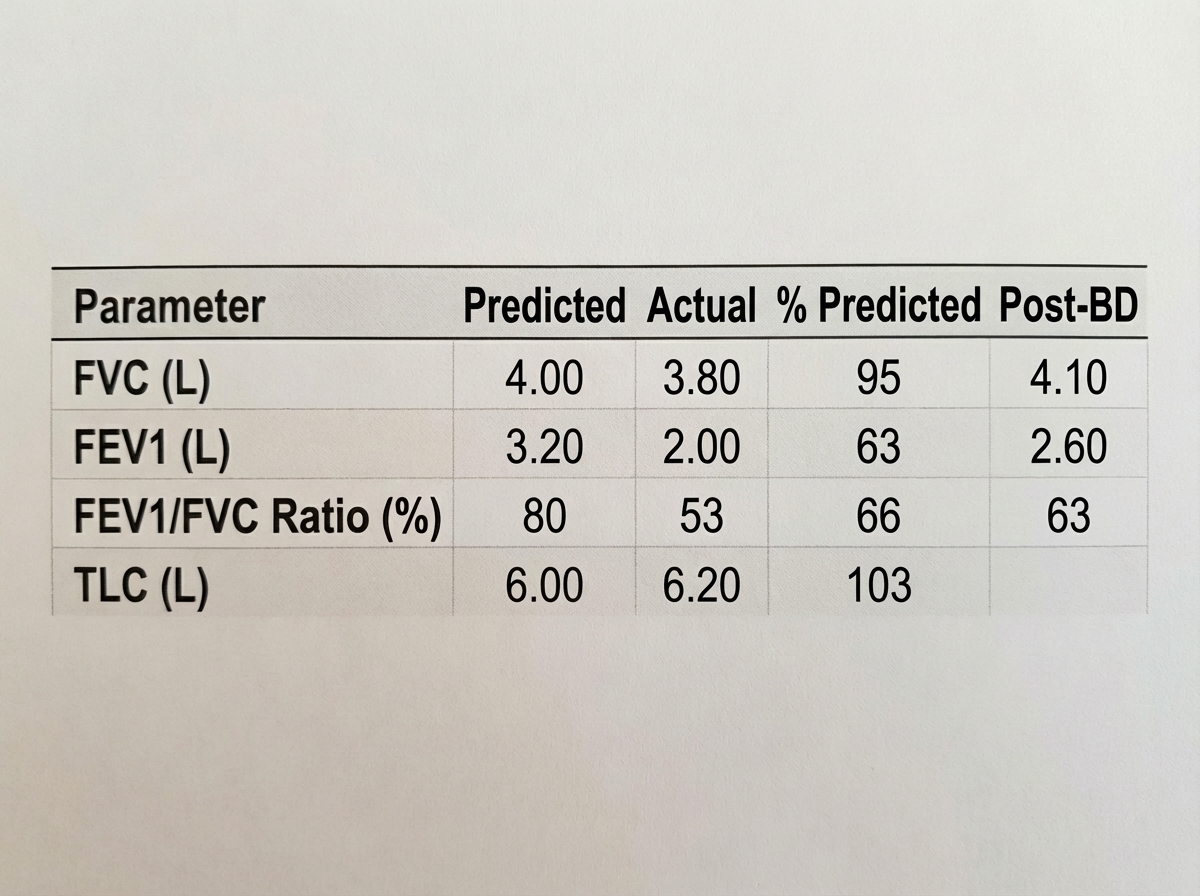
Based on the provided pulmonary function test results, what is the most likely diagnosis?
What is the most common ECG change in pulmonary embolism?
Which of the following are risk factors for pulmonary embolism?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app