
Bronchiectasis and Cystic Fibrosis — MCQs

Cystic fibrosis leads to defect in which of the following channels?
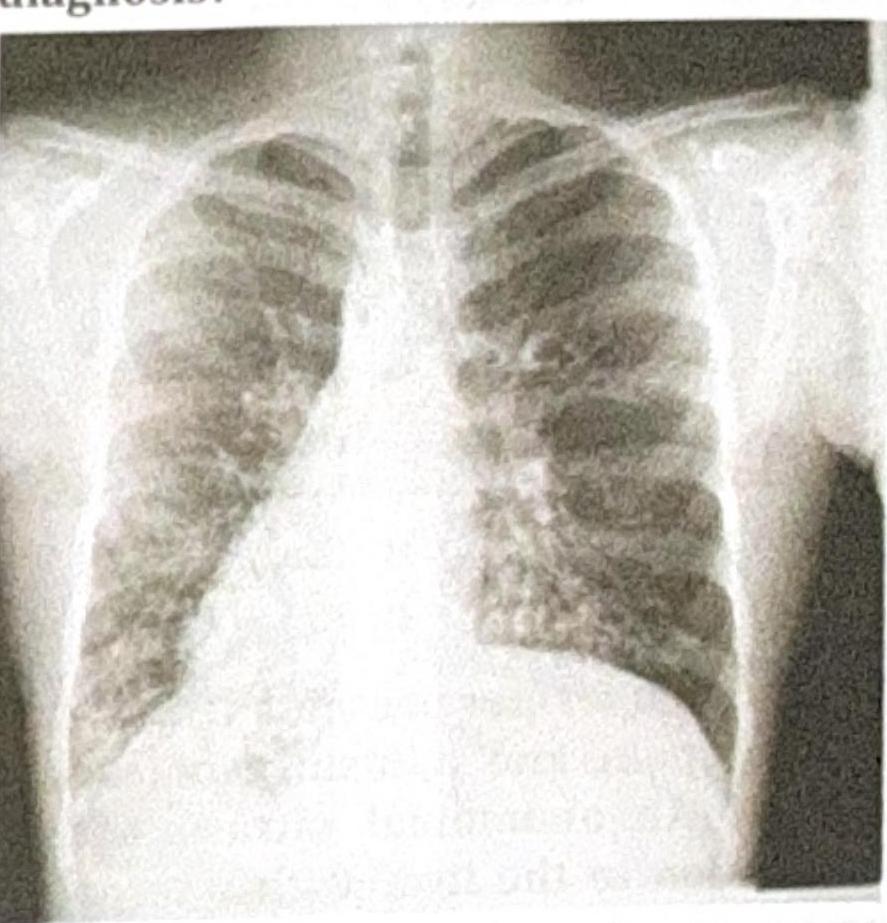
A 40-year-old man presented with repeated episodes of bronchospasm and hemoptysis. Chest X-ray revealed perihilar bronchiectasis. The most likely diagnosis is
In bronchiectasis, all of the following are seen except:
Ring sign with dilated bronchi on CXR is a feature of
Chloride level in sweat is used in the diagnosis of which disease?
Which of the following is not typically associated with cystic fibrosis?
A 3-year-old child is evaluated by a pediatrician for poor growth despite excessive food intake. The mother reports that the child's stools are bulky, foul-smelling, and difficult to flush because they float. Determination of which of the following would most likely be diagnostic in this case?
Investigation of choice in bronchiectasis?
A patient presents with recurrent lung infections, and the chest X-ray provided shows a characteristic finding. What is the most likely diagnosis?
Post-tubercular bronchiectasis is most commonly seen with
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app