
Pulmonology — MCQs

On this page
A trekker at high altitude develops ataxia and confusion, followed by pulmonary edema. What is the most appropriate management?
A 60-year-old female presents with chronic breathlessness and cough for several years, which has progressively worsened. She has a significant smoking history of 30 pack-years. There is no history of atopy. Pulmonary function testing shows a post-bronchodilator FEV/FVC ratio of <0.7 with an 18% improvement in FEV1 after bronchodilator administration. CXR is shown below?
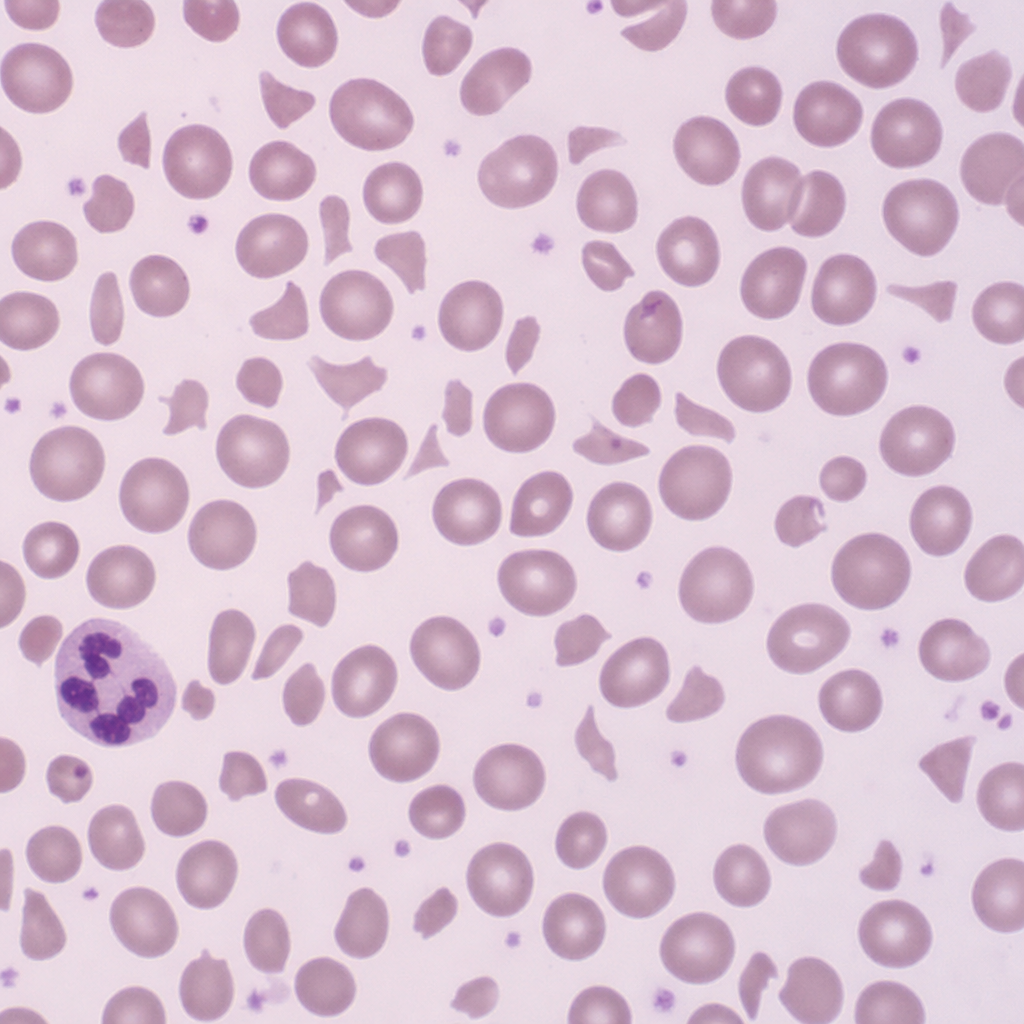
A 32-year-old woman presents with a 5-day history of confusion, fever, and oliguria. Laboratory results show haemoglobin 7.2 g/dL, platelets 18,000/µL, creatinine 2.8 mg/dL, and markedly elevated LDH. Her coagulation profile (PT, aPTT, fibrinogen) is within normal limits. A peripheral blood smear is shown (Image 1). Which of the following is the most appropriate immediate intervention?
The blood gas parameters: pH 7.58, pCO2 23 mm Hg, pO2 300 mm Hg, and oxygen saturation 60% are most consistent with which of the following?
A 24-year-old woman presents with increasing shortness of breath following treatment for right lower lobe pneumonia. She denies fever, cough, or sputum production. Examination reveals decreased tactile fremitus, dullness to percussion, and absent breath sounds over the right lower lung. Additionally, the trachea is deviated to the left. What is the most likely diagnosis for this patient's abnormal pulmonary physical findings?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app