
Nephrology — MCQs

On this page
A diabetic patient presents with hyperkalemia and urinary pH < 5.5. What is the MOST likely underlying cause?
Interstitial nephritis is common with
Which of the following is not an absolute indication for hemodialysis?
Which of the following is a characteristic finding in distal RTA?
Which of the following is a sign of Bartter's syndrome?
What is the expected Transtubular Potassium Gradient (TTKG) in a patient with hypokalemia due to extrarenal losses?
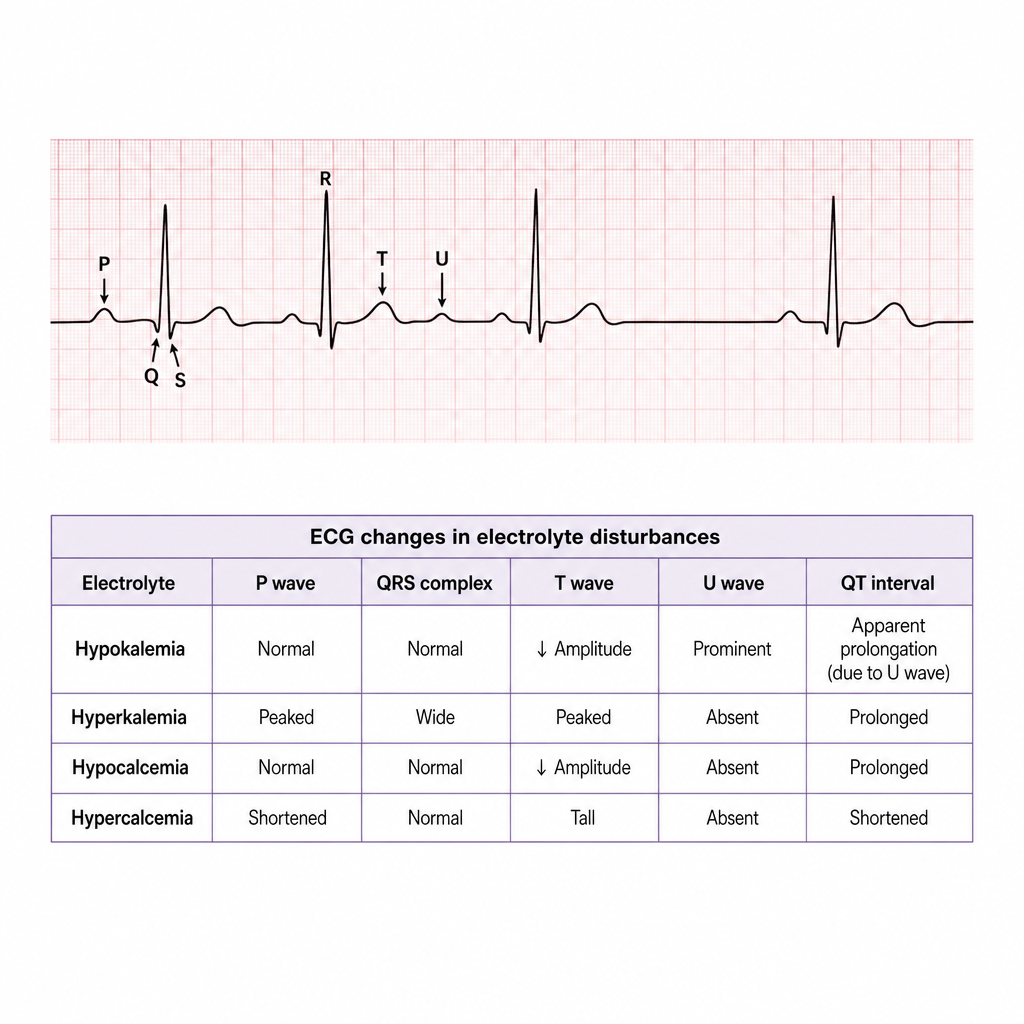
ECG image showing U wave. Patient is on furosemide and beta blocker. What is the most likely diagnosis?
What is the recommended rate of correction for sodium deficit in patients with chronic hyponatremia?
Which of the following statements about HIV associated nephropathy (HIVAN) is incorrect?
Which of the following is not a typical feature of haemolytic uremic syndrome?
Practice by Chapter
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Glomerular Diseases
Practice Questions
Tubulointerstitial Diseases
Practice Questions
Nephrotic and Nephritic Syndromes
Practice Questions
Urinary Tract Infections
Practice Questions
Renal Replacement Therapy
Practice Questions
Fluid and Electrolyte Disorders
Practice Questions
Acid-Base Disorders
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Kidney Stones and Obstructive Uropathy
Practice Questions
Hypertension in Kidney Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app