
Nephrology — MCQs

On this page
Hypomagnesemia is associated with which of the following electrolyte imbalances?
Which disease recurs after kidney transplantation?
A 72-year-old man develops acute renal failure following aortic angiography. He has gained weight, has rales at both lung bases, and is dyspneic. His fractional excretion of sodium is greater than 1. Peripheral smear shows eosinophilia, and his labs reveal an elevated erythrocyte sedimentation rate, proteinuria, and microscopic hematuria. What is the most likely cause of his renal failure?
What is the new indication of tolvaptan as approved by FDA recently?
What is the best prophylactic drug for a 60-year-old asthmatic female with microalbuminuria of 280mg?
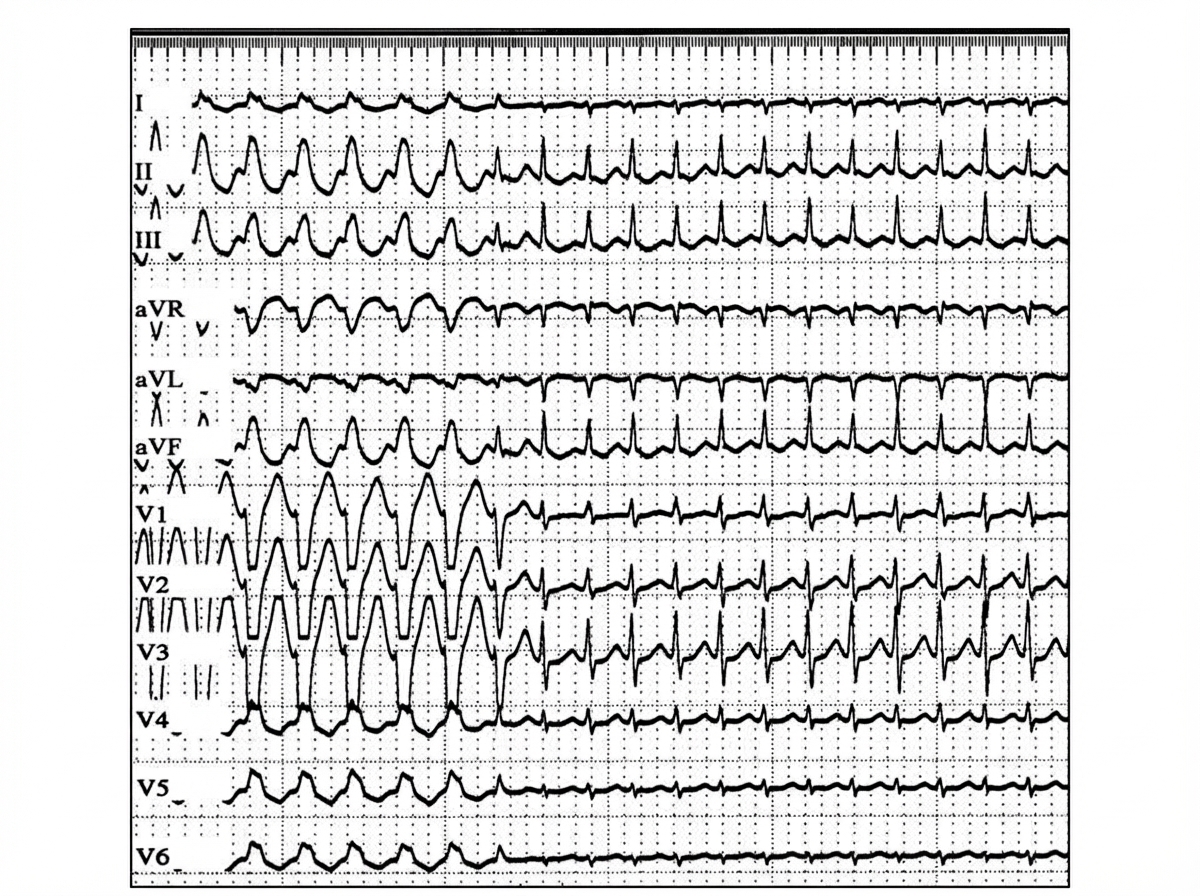
A 43-year-old woman develops acute renal failure following an emergency resection of a leaking abdominal aortic aneurysm. One week after surgery, the following laboratory values are obtained: Serum electrolytes (mEq/L): Na+ 127, K+ 5.9, Cl- 92, HCO3- 15. Blood urea nitrogen: 82 mg/dL. Serum creatinine: 6.7 mg/dL. The patient has gained 4 kg since surgery and is mildly dyspneic at rest. Eight hours after these values are reported, the following electrocardiogram is obtained. Which of the following is the most appropriate initial treatment in the management of this patient?
What is the earliest sign of hyperkalemia on an ECG?
Hypokalemia is seen in all the following conditions except?
Renal Tubular Acidosis (RTA) shows all except?
Which of the following is true about nephrogenic diabetes insipidus?
Practice by Chapter
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Glomerular Diseases
Practice Questions
Tubulointerstitial Diseases
Practice Questions
Nephrotic and Nephritic Syndromes
Practice Questions
Urinary Tract Infections
Practice Questions
Renal Replacement Therapy
Practice Questions
Fluid and Electrolyte Disorders
Practice Questions
Acid-Base Disorders
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Kidney Stones and Obstructive Uropathy
Practice Questions
Hypertension in Kidney Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app