
Nephrology — MCQs

On this page
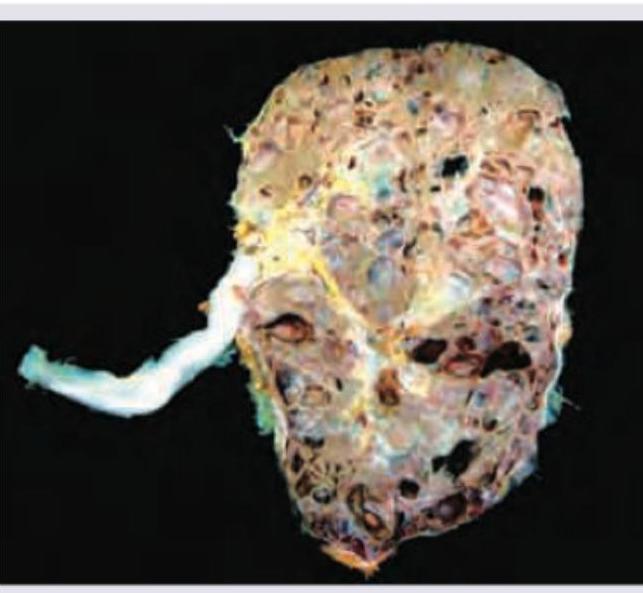
All are true about the condition shown in the above figure except:
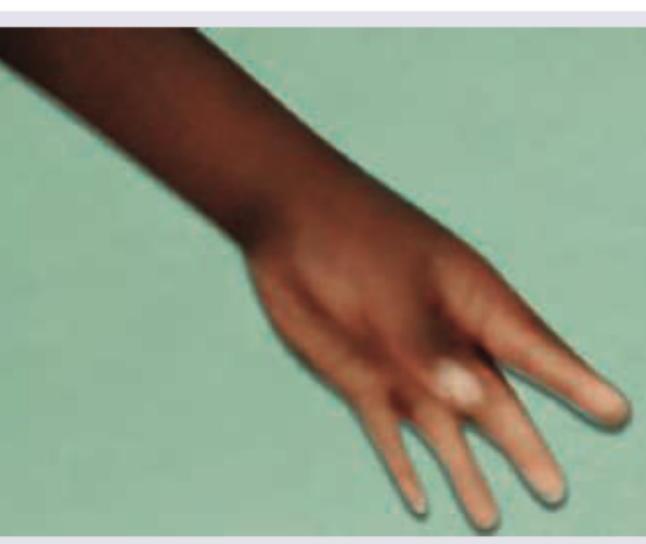
The hand of a patient of Gitelman syndrome shows?
Hemodialysis is being performed on a patient of ESRD. Central dialysis catheter is placed at which site?

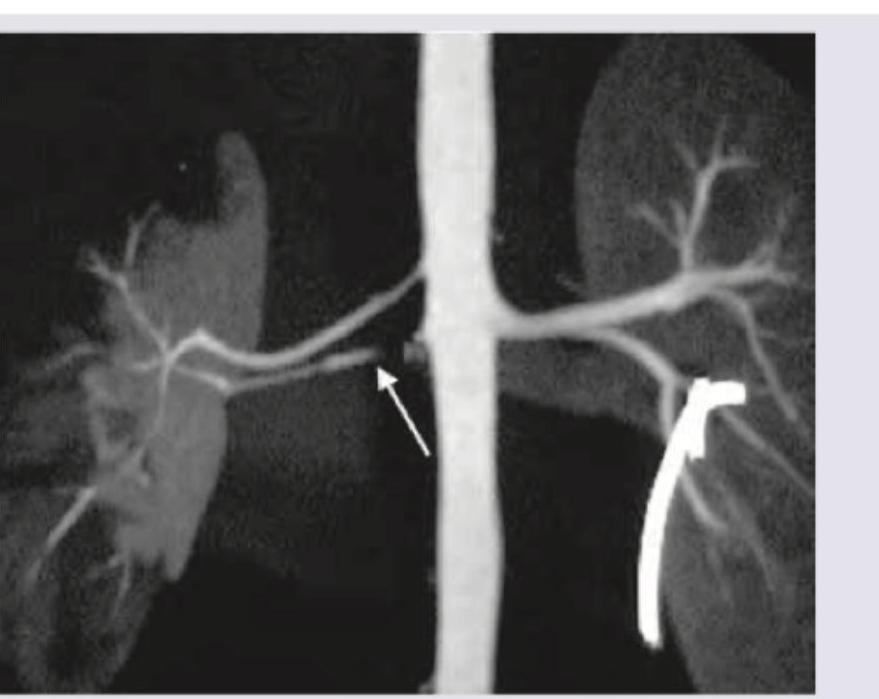
A 60-year-old hypertensive patient was showing poor response to three classes of antihypertensive drugs (ACE inhibitors, CCB and diuretics). Renal CT angiography was performed. What is the diagnosis?
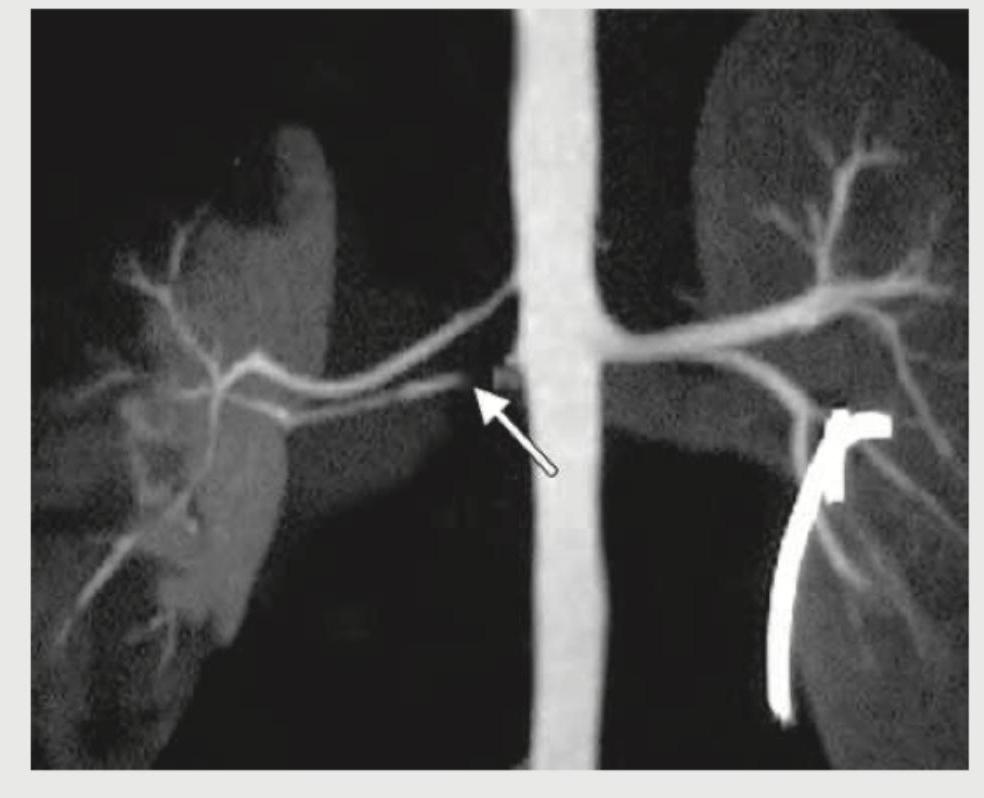
Most common cardiovascular association of this disease leading to mortality is:
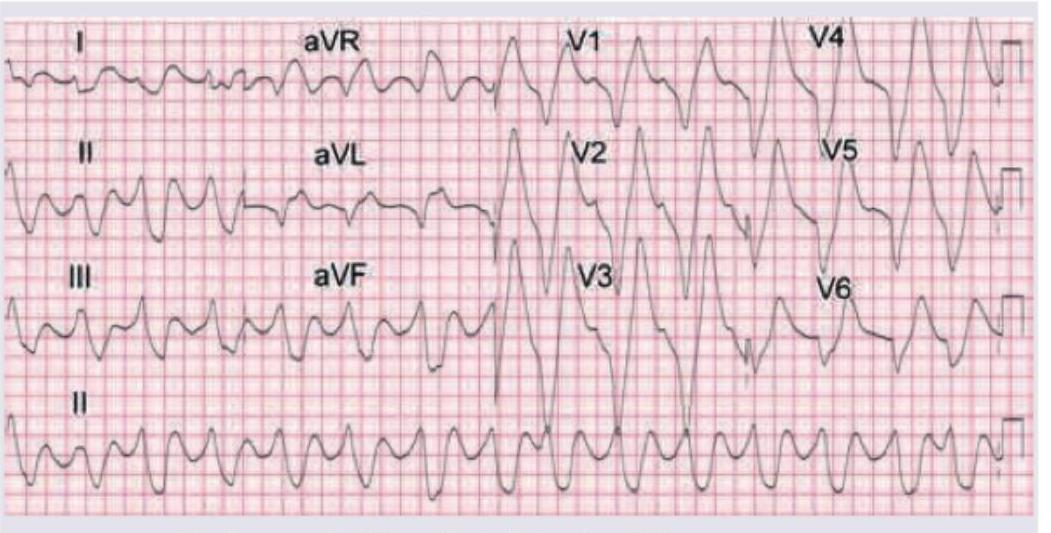
A patient of ESRD is scheduled for hemodialysis. He complains of palpitations. Which of the following findings are seen on ECG?
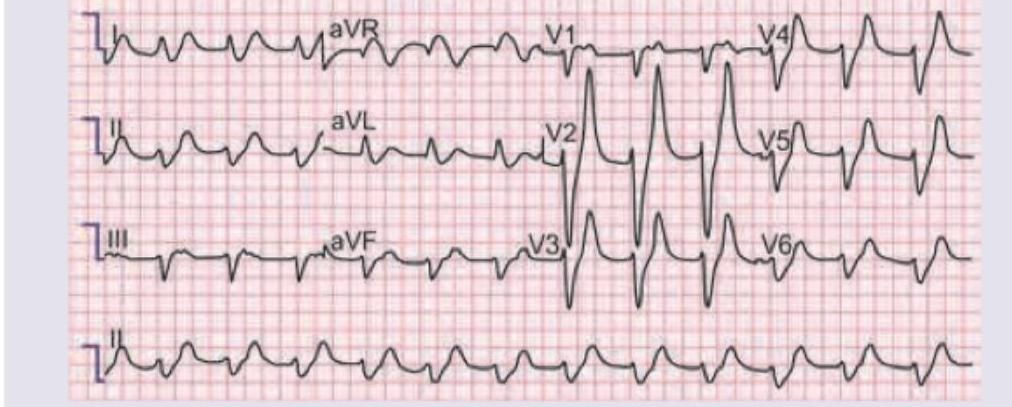
A 30-year-old lady with crush injury was admitted to the casualty. Her urobag shows 100 mL red color urine. Serum potassium is 6.8 mEq/L, creatinine is 4.2 mg/dL, and urine output over the past 2 hours is 20 mL. She has not responded to initial medical therapy. ECG is shown below. All are indicated for this patient except?
Which of the following findings in a patient are suggestive of acute nephritis? I. Hematuria II. Oliguria III. Reduced size of both kidneys IV. Edema Select the correct answer using the code given below :
Which one of the following hereditary tubulo-interstitial kidney diseases has an autosomal recessive mode of inheritance?
Kidney damage and Glomerular Filtration Rate (GFR) value between 15-29 mL / min / 1.73 m^2 are found in which stage of Chronic Kidney Disease?
Practice by Chapter
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Glomerular Diseases
Practice Questions
Tubulointerstitial Diseases
Practice Questions
Nephrotic and Nephritic Syndromes
Practice Questions
Urinary Tract Infections
Practice Questions
Renal Replacement Therapy
Practice Questions
Fluid and Electrolyte Disorders
Practice Questions
Acid-Base Disorders
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Kidney Stones and Obstructive Uropathy
Practice Questions
Hypertension in Kidney Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app