
Nephrology — MCQs

On this page
Which of the following is not a cause of high anion gap metabolic acidosis?
A 60-year-old man with chronic kidney disease presents with complaints of increasing fatigue, dyspnea on exertion, and signs of congestive heart failure. On evaluation, he is found to have anemia. What is the most appropriate next step in management?
A 55-year-old man presents with altered sensorium and deep labored breathing. ABG is given below. What is the most likely acid-base disorder? pH: 7.20 pCO₂: 31 mmHg HCO₃⁻:16 mEq/L Na⁺: 130 mEq/L Cl⁻: 84 mEq/L PaO₂: 80 mmHg
A 68-year-old male with a history of COPD presents to the emergency room with severe dyspnea and altered mental status. An arterial blood gas (ABG) is drawn with the following results: pH: 7.28 PaCO2: 60 mmHg HCO3-: 28 mEq/L Na+: 142 mEq/L Cl-: 100 mEq/L Based on these results, what is the calculated anion gap?
Patient came with severe headache and seizures. Sodium on admission was 98 meq/L. We have started correction with 3 % saline and now after 24 hours of infusion sodium is 110 meq/L. Patient develops mutism and altered sensorium. Which investigation will you perform now?
Which of the following is not a recognised cause of recurrent renal stone formation?
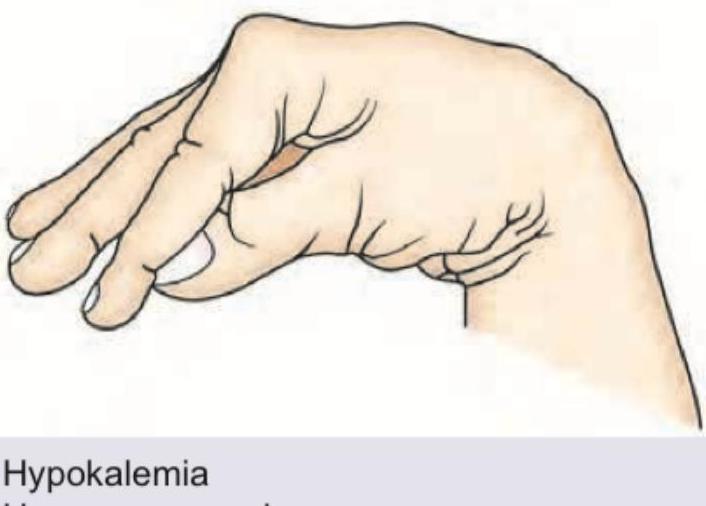
Which is correct about the sign shown?
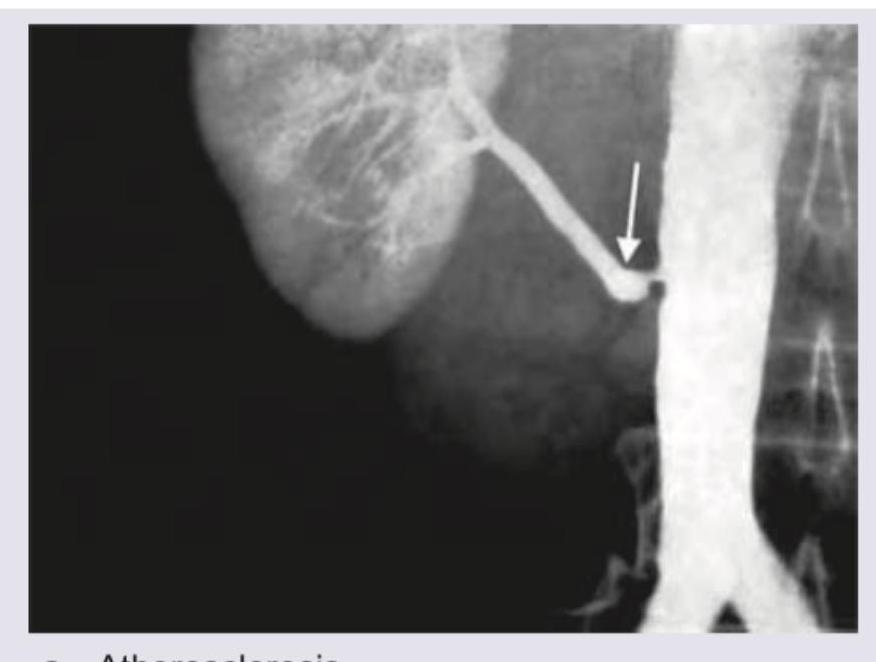
A 45-year-old male patient with a history of smoking over 20 years develops hypertension renal angiography was performed. The most common cause for this condition is?
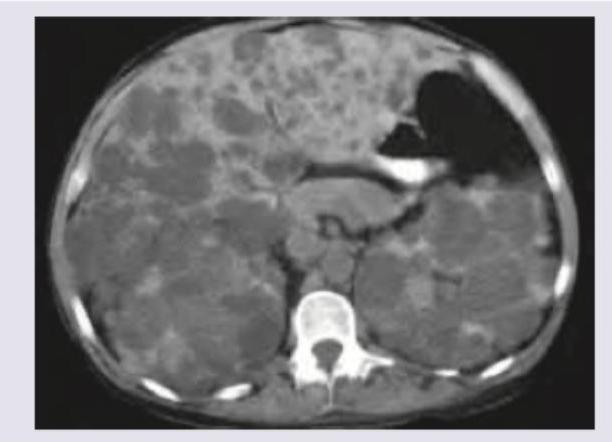
A 30-year-old hypertension patient presents with flank pain. CT abdomen was performed. All are true about the condition shown except?
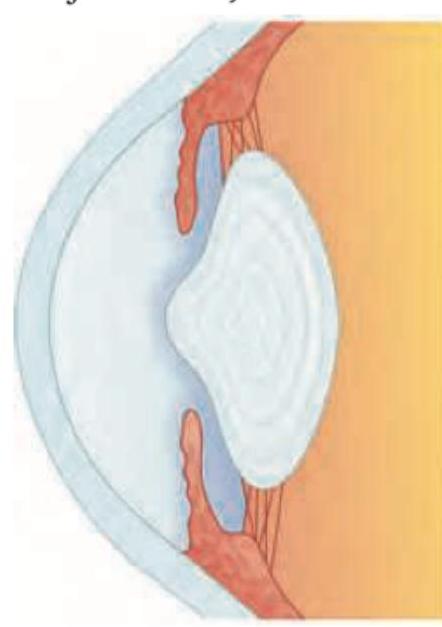
A patient presents with recurrent episodes of gross hematuria, anterior lenticonus (as shown in the image), and sensorineural deafness. Which diagnosis is most likely?
Practice by Chapter
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Glomerular Diseases
Practice Questions
Tubulointerstitial Diseases
Practice Questions
Nephrotic and Nephritic Syndromes
Practice Questions
Urinary Tract Infections
Practice Questions
Renal Replacement Therapy
Practice Questions
Fluid and Electrolyte Disorders
Practice Questions
Acid-Base Disorders
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Kidney Stones and Obstructive Uropathy
Practice Questions
Hypertension in Kidney Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app