
Nephrology — MCQs

On this page
Which of the following is NOT an indication for dialysis in a case of acute renal failure?
Fluid containing which of the following substances is used in peritoneal dialysis?
Calciphylaxis is more commonly seen in which of the following conditions?
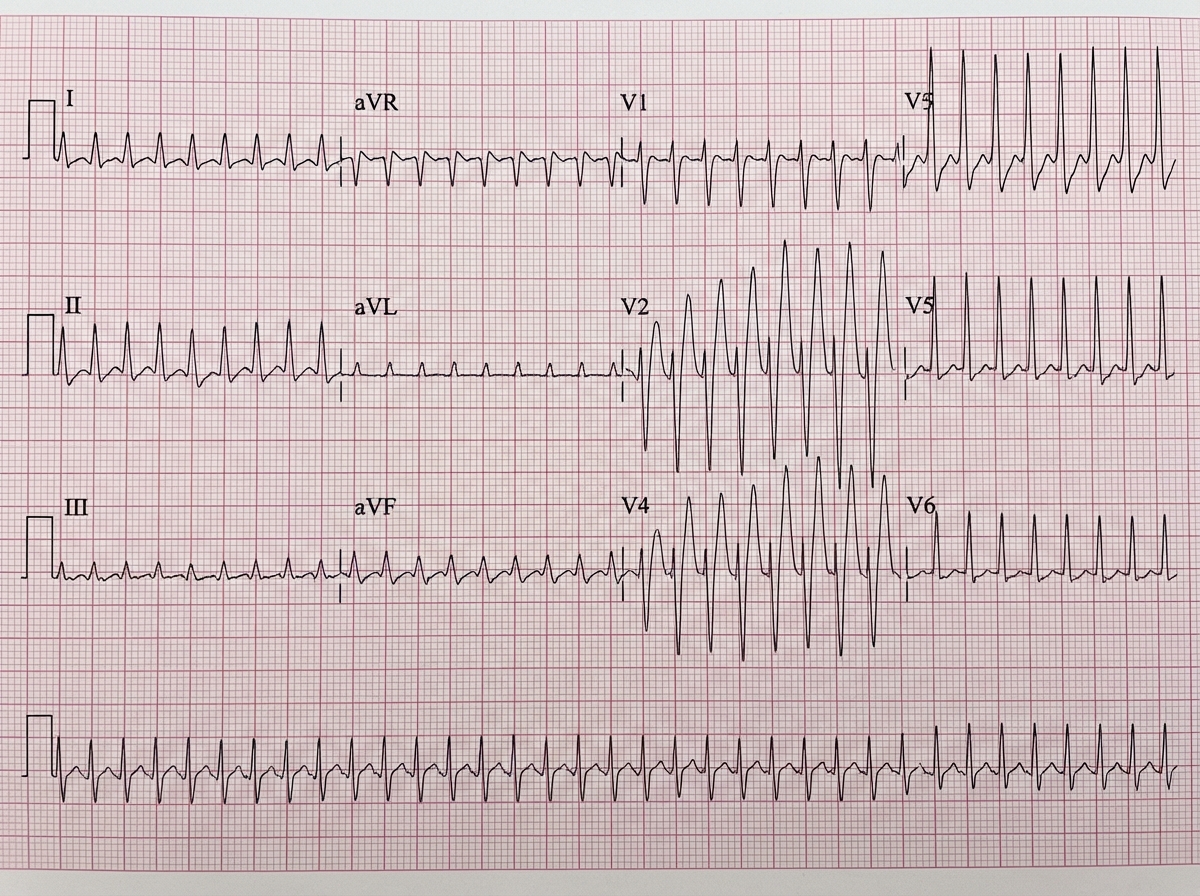
A 14-year-old boy was brought in a collapsed state with a history of 2 episodes of vomiting and presented with a feeble pulse and cold, clammy limbs. ECG is provided. What is the diagnosis?
A normal anion gap metabolic acidosis occurs in patients with which of the following conditions?
Which of the following is a true complication of hemodialysis?
A patient presents with hyperkalemia and no ECG changes. Which of the following is used for treatment, EXCEPT?
A 58-year-old man with cirrhosis complains of worsening fatigue and confusion over the past 5 days. He also reports a declining urinary output over the past 48 hours. On examination, he is gaunt and jaundiced. He has tense ascites and a liver span of 7 cm in the midclavicular line. Lab results reveal a WBC 4600/mm3, Hb 9.4 g/dL, and PCB 29%. BUN of 34 mg/dL and a creatinine of 3.1 mg/dL. A urinary Na <10 mEq/L. What is the most appropriate treatment for his elevated BUN and creatinine?
A 25-year-old man presents with a kidney stone. He is married to his first cousin, and six months earlier, his 8-year-old son also had a kidney stone. What is the most likely diagnosis?
What is the cornerstone of therapy for chronic hyponatremia?
Practice by Chapter
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Glomerular Diseases
Practice Questions
Tubulointerstitial Diseases
Practice Questions
Nephrotic and Nephritic Syndromes
Practice Questions
Urinary Tract Infections
Practice Questions
Renal Replacement Therapy
Practice Questions
Fluid and Electrolyte Disorders
Practice Questions
Acid-Base Disorders
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Kidney Stones and Obstructive Uropathy
Practice Questions
Hypertension in Kidney Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app