
Nephrology — MCQs

On this page
The primary cause of anemia in chronic kidney disease (CKD) is:
A 40-year-old diabetic woman complains of flank pain and fever. Her temperature is 38.7°C, respirations are 25 per minute, and blood pressure is 150/90 mm Hg. Urinalysis reveals pyuria with WBC casts. Which of the following features of diabetes is the most important contributing factor in the development of flank pain and fever in this patient?
A 56-year-old man presents with hypertension and peripheral edema. He is otherwise healthy and takes no medications. Family history reveals that his father and a brother have kidney disease. His father was on hemodialysis before his death at age 68 of a stroke. Physical examination reveals BP 174/96 and AV nicking on funduscopic examination. He has a soft S4 gallop. Bilateral flank masses measuring 16 cm in length are palpable. Urinalysis shows 15 to 20 RBC/hpf and trace protein but is otherwise normal; his serum creatinine is 2.4 mg/dL. Which is the most likely long-term complication of his condition?
Dialysis is not indicated in which of the following conditions?
What is the initial treatment of choice for a patient with chronic kidney disease and hypertension?
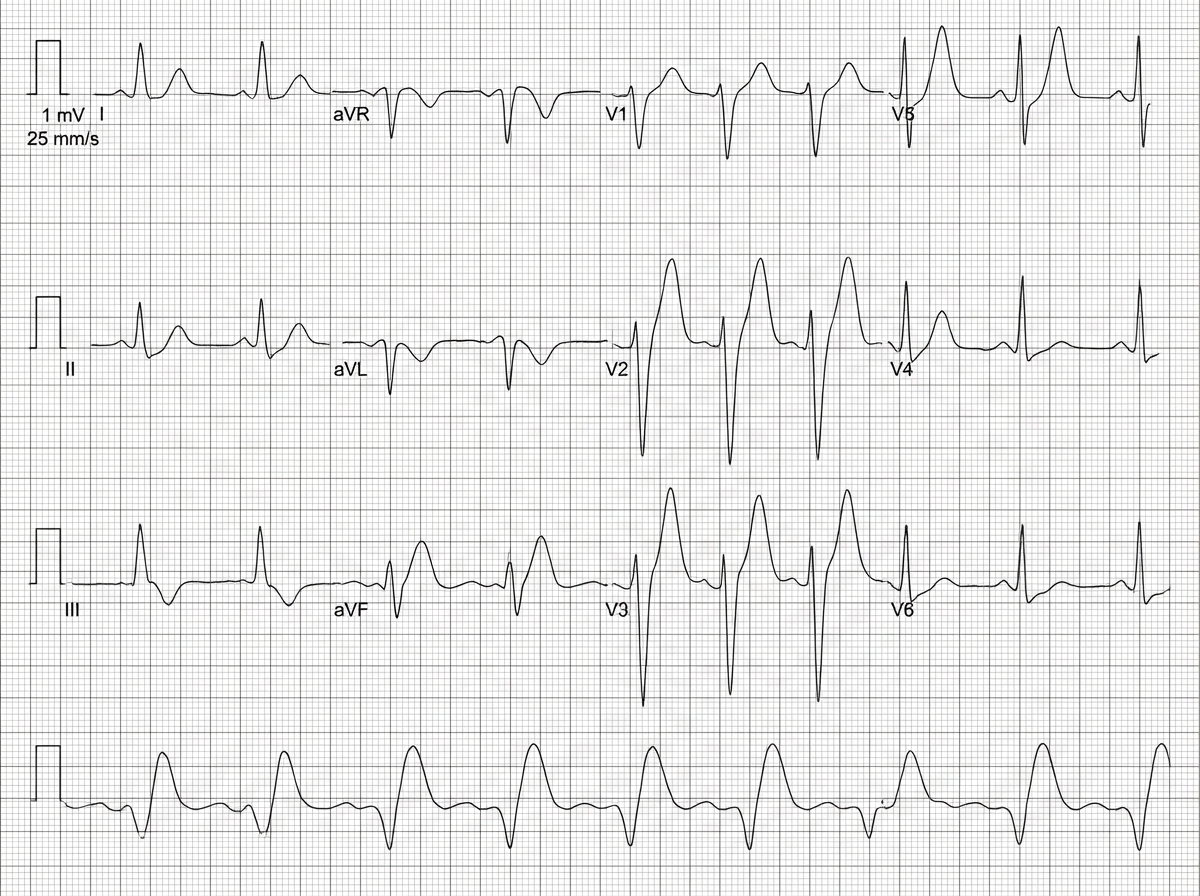
A patient presents to the emergency department in an unconscious state after a 15-minute delay following a call. The patient has a barely palpable radial pulse and no signs of trauma. The systolic blood pressure is 58 mm Hg. An ECG is shown. Which electrolyte abnormality is most likely to cause this clinical scenario?
Renal artery stenosis is associated with which of the following?
Metabolic complications in chronic renal failure (CRF) include all of the following EXCEPT?
All of the following are indicated in the management of acute hyperkalemia except?
Which of the following conditions causes euvolemic hyponatremia?
Practice by Chapter
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Glomerular Diseases
Practice Questions
Tubulointerstitial Diseases
Practice Questions
Nephrotic and Nephritic Syndromes
Practice Questions
Urinary Tract Infections
Practice Questions
Renal Replacement Therapy
Practice Questions
Fluid and Electrolyte Disorders
Practice Questions
Acid-Base Disorders
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Kidney Stones and Obstructive Uropathy
Practice Questions
Hypertension in Kidney Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app