
Nephrology — MCQs

On this page
What is the cause of hypercoagulation in nephrotic syndrome?
What is the most rapid method for lowering serum potassium levels?
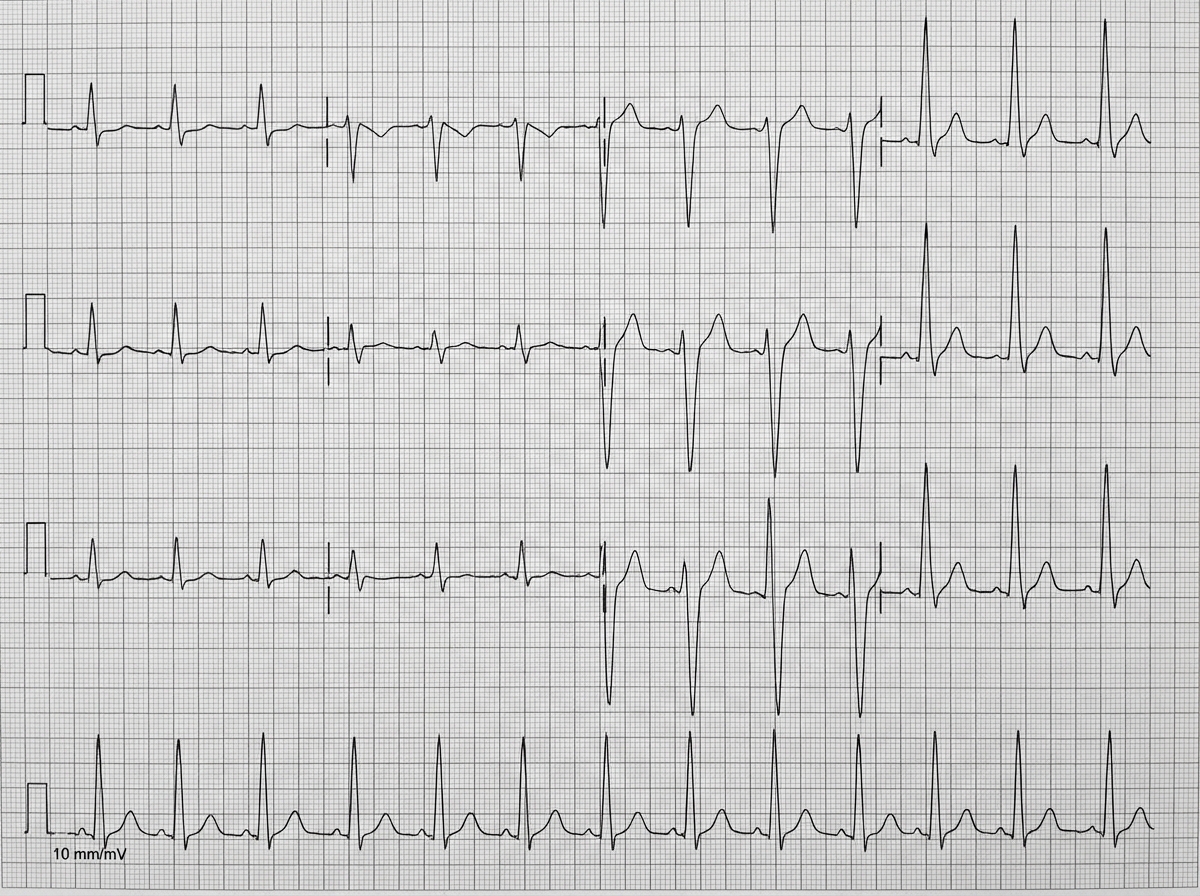
A 78-year-old man with chronic kidney disease presents with generalized malaise. His past medical history includes heart failure, hypertension, and type 2 diabetes. Medications are ramipril, insulin, furosemide, and metoprolol. On physical examination, the blood pressure is 155/90 mm Hg, heart rate is 100/min, and respiration 24/min. The heart sounds are normal, there is no edema, and the lungs are clear on auscultation. An ECG is performed. What is the most likely diagnosis based on the ECG findings?
Hyperkalemia is seen in which type of Renal Tubular Acidosis?
Proximal renal tubular acidosis has all the following features except?
Which of the following statements regarding high anion gap is FALSE?
Broad casts in urinary sediments are specific for:
What is the primary diagnostic laboratory finding in nephrotic syndrome?
A patient with autosomal dominant polycystic kidney disease (ADPKD) is taking tolvaptan and is complaining of abdominal pain and loose stools. What is the likely cause of these symptoms?
During a routine physical examination, a 42-year-old female is found to have an elevated blood pressure of 150/100 mmHg. Workup reveals a small left kidney and a normal-sized right kidney. Laboratory examination reveals elevated serum renin levels, and renal vein renin levels are increased on the left but decreased on the right. This patient's hypertension is most likely the result of?
Practice by Chapter
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Glomerular Diseases
Practice Questions
Tubulointerstitial Diseases
Practice Questions
Nephrotic and Nephritic Syndromes
Practice Questions
Urinary Tract Infections
Practice Questions
Renal Replacement Therapy
Practice Questions
Fluid and Electrolyte Disorders
Practice Questions
Acid-Base Disorders
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Kidney Stones and Obstructive Uropathy
Practice Questions
Hypertension in Kidney Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app