
Nephrology — MCQs

On this page
All of the following antibiotics are known to cause acute interstitial nephritis, except?
A 55-year-old man with type II diabetes mellitus, essential hypertension, and ischemic heart disease presents for a routine examination. Laboratory studies reveal a serum potassium of 6 mEq/L. He has no muscle weakness and no ECG changes apart from evidence of a prior inferior wall myocardial infarction. He has mild compensated metabolic acidosis with a normal serum anion gap. Urine examination shows significantly lower than expected potassium excretion despite an elevated serum potassium concentration. Which of the following is most likely to explain the hyperkalemia observed in this patient?
Increased anion gap acidosis is seen in which of the following conditions?
Which investigation should be avoided in a proven case of renal papillary necrosis?
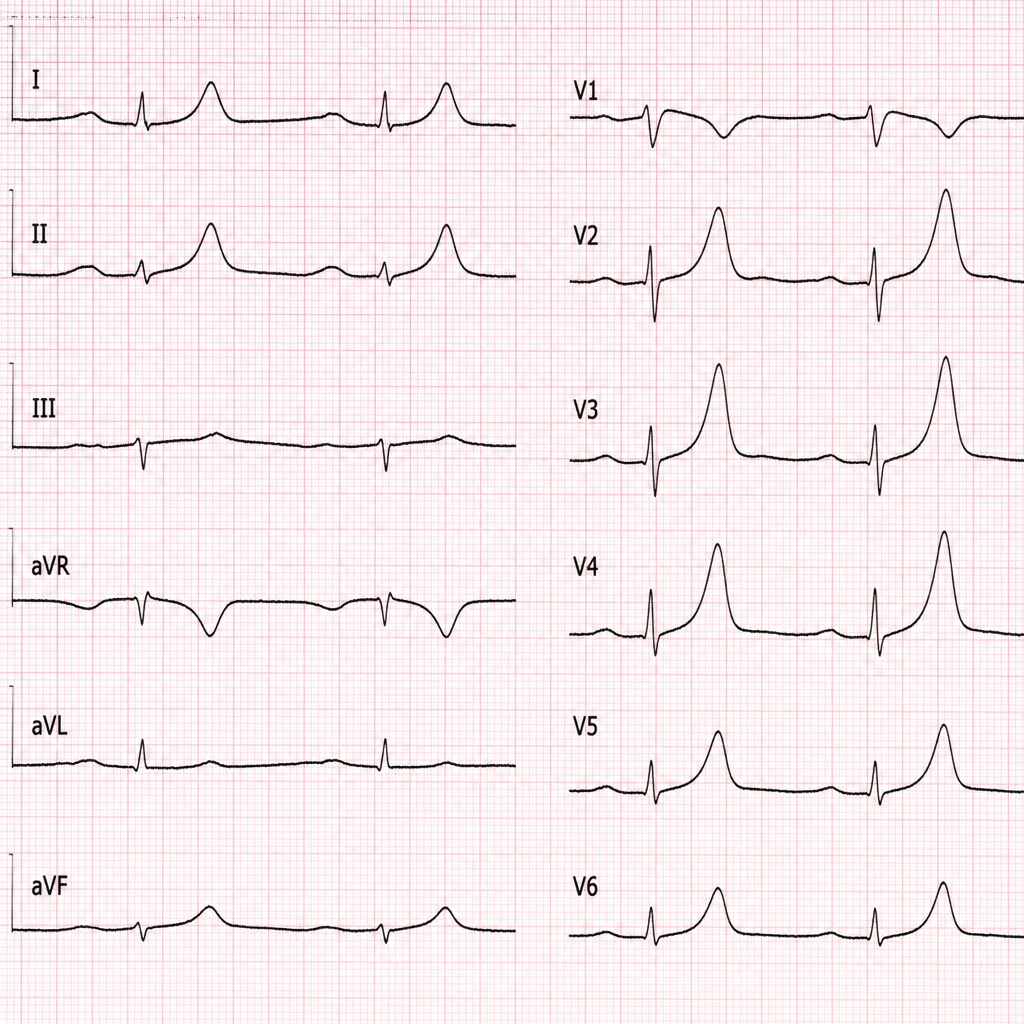
Which of the following conditions is characterized by these ECG changes?
Which of the following conditions is NOT associated with hypokalemia and hypertension?
In which one of the following conditions is a renal biopsy contraindicated?
Which of the following is a common feature of Gitelman syndrome?
Pre-renal azotemia is associated with which of the following characteristic features?
What is the most common organism isolated in emphysematous pyelonephritis?
Practice by Chapter
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Glomerular Diseases
Practice Questions
Tubulointerstitial Diseases
Practice Questions
Nephrotic and Nephritic Syndromes
Practice Questions
Urinary Tract Infections
Practice Questions
Renal Replacement Therapy
Practice Questions
Fluid and Electrolyte Disorders
Practice Questions
Acid-Base Disorders
Practice Questions
Kidney in Systemic Diseases
Practice Questions
Kidney Stones and Obstructive Uropathy
Practice Questions
Hypertension in Kidney Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app