
Hematology — MCQs

On this page
Which of the following are blood values of Iron Deficiency Anaemia ? 1. Serum iron is less than 30 mg/100 mL 2. Total iron binding capacity is less than 400 µg/mL 3. Percentage saturation is 10% or less 4. Serum ferritin is below 30 µg/mL Select the correct answer using the code given below :
Which of the following statements are correct regarding iron deficiency? 1. More common in older age group 2. More common in females of reproductive age 3. Associated with heavy menstrual bleeding 4. Commonly caused by chronic blood loss Select the correct answer using the code given below.
Which of the following statements are correct in respect of haemophilia? 1. It is hereditary bleeding disorder. 2. It has a higher incidence among Asians. 3. It affects females occasionally and mildly.
The following are the common features of Idiopathic Thrombocytopenic Purpura except
Priapism in a young male could occur because of
Umbilical cord blood stem cells are used to treat all the following diseases except :
Consider the following statements: Haemophilia A (haemophilia) and Haemophilia B (christmas disease) 1. are variants of the same disease process 2. are due to congenital deficiency of factor VIII and factor IX respectively 3. both are sex linked characteristics and transmitted by asymptomatic females 4. can occur both in males and females Select the correct answer using the code given below:
The ideal temperature to store the whole blood in blood-bank is
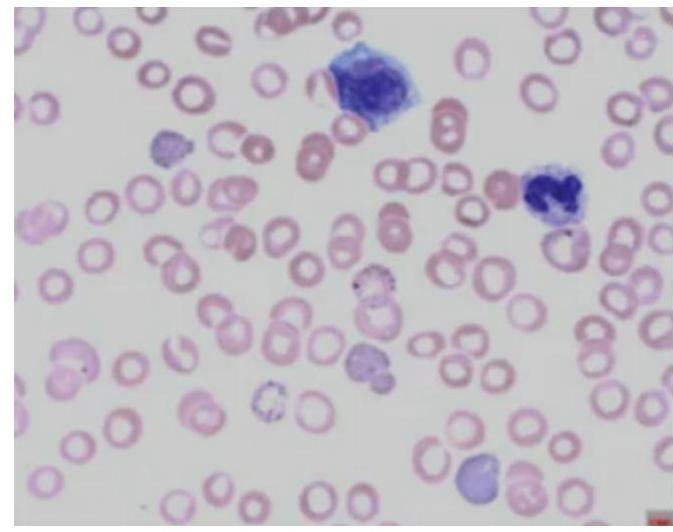
Which of the following diagnoses give the hematological picture as given below?
Which of the following statements is correct about Paroxysmal Nocturnal Hemoglobinuria (PNH)?
Practice by Chapter
Anemia Evaluation and Management
Practice Questions
Hemoglobinopathies
Practice Questions
Thalassemias
Practice Questions
Platelet Disorders
Practice Questions
Coagulation Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Leukemias
Practice Questions
Lymphomas
Practice Questions
Multiple Myeloma and Plasma Cell Disorders
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Transfusion Medicine
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app