
Hematology — MCQs

On this page
Which of the following statements is not true regarding hemophilia A?
Platelet function defect is seen in which of the following conditions?
A 19-year-old college student develops a severe sore throat, cervical lymphadenopathy, and atypical lymphocytes on blood film. A heterophil antibody test is positive. For the above patient with a hematologic abnormality, select the most likely diagnosis.
What is the recommended daily amount of elemental iron required for iron replacement therapy?
While managing a febrile neutropenic patient, all of the following are essential EXCEPT:
Which of the following statements is true regarding oral therapy for iron deficiency anemia?
All of the following statements about hereditary hemochromatosis are true EXCEPT?
Aplastic anemia is characterized by which of the following findings?
Which of the following is a major criterion for the diagnosis of polycythemia vera?
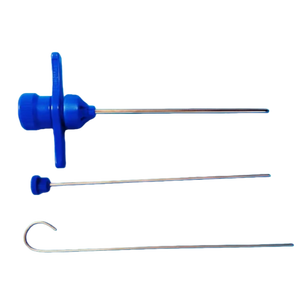
For which procedure is the following instrument used?
Practice by Chapter
Anemia Evaluation and Management
Practice Questions
Hemoglobinopathies
Practice Questions
Thalassemias
Practice Questions
Platelet Disorders
Practice Questions
Coagulation Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Leukemias
Practice Questions
Lymphomas
Practice Questions
Multiple Myeloma and Plasma Cell Disorders
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Transfusion Medicine
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app