
Hematology — MCQs

On this page
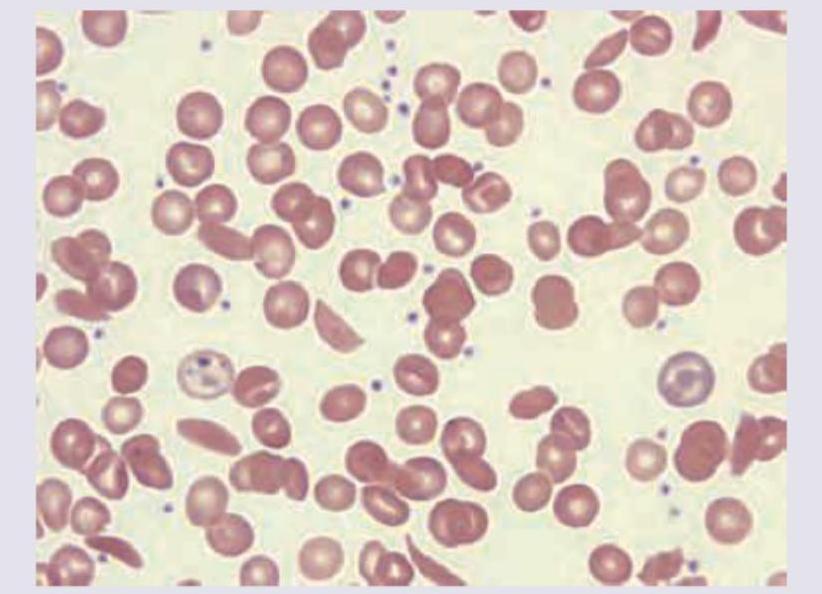
A 16-year-old boy presents with jaundice and splenomegaly. His father had a similar illness during adolescence. MCHC : high? What is the most likely diagnosis?
Which of the following is the most common inherited bleeding disorder?
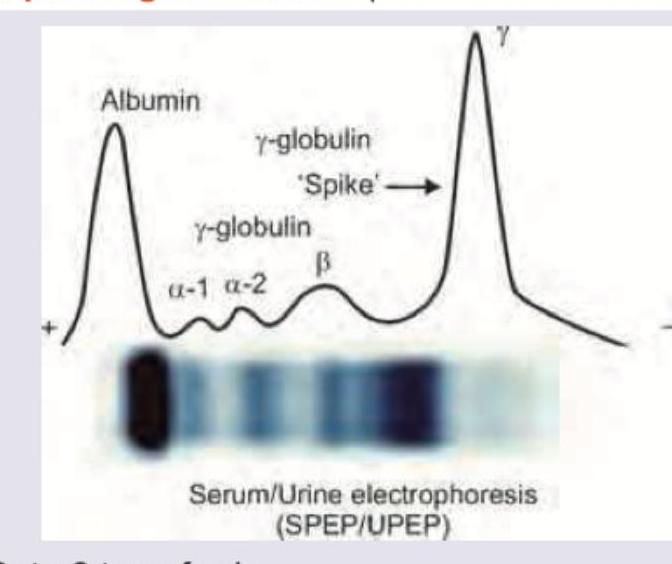
A 40-year-old patient presents with complains of low back pain and development of pallor. During workup very high levels of urinary beta2 microglobulin was noted. X-ray skull was performed. Bone marrow aspiration shows >10% plasma cells and serum electrophoresis shows M protein >30 g/L. All are useful for management of this patient except?
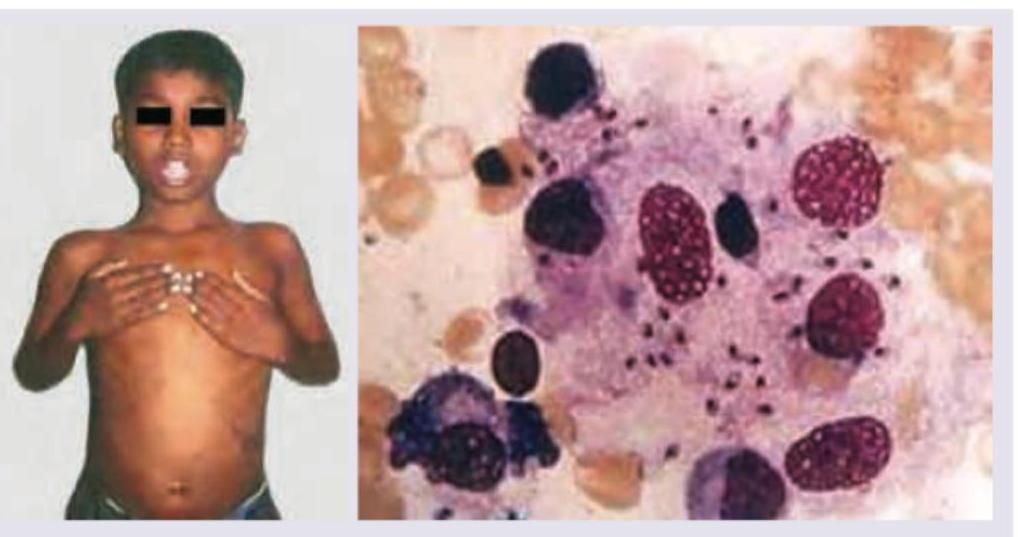
Comment on the diagnosis in the patient shown below?
An 8-year-old child of migrant construction worker presents with fever for last 2 weeks with progressive pallor. Complete blood counts reveal pancytopenia, malaria work up is negative, Total serum protein is 7 gm% with Serum Globulin of 4.5 gm%, serum albumin 3.5 mg%. Bone marrow study shows?
What is the threshold for prophylactic administration of the following blood product?

A patient in ICU was given blood transfusion. 3 hours later SpO2 is reduced to 75% with respiratory difficulty. CVP is 15 cm water and PCWP is 25 mm Hg . CXR is shown below. What is the diagnosis?

Which of the following is a prognostic marker for the patient whose urinary and serum electrophoresis report is given below?
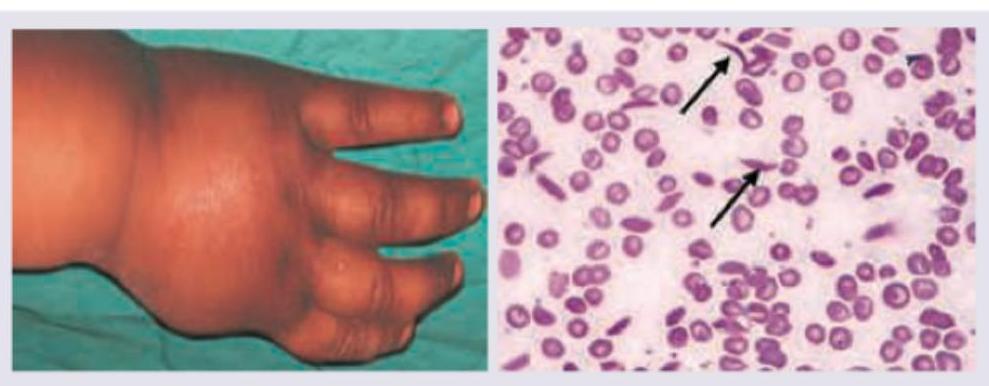
The patient with the following hematological abnormality presents with severe chest pain and difficulty in breathing. All are useful for managing this emergency except:
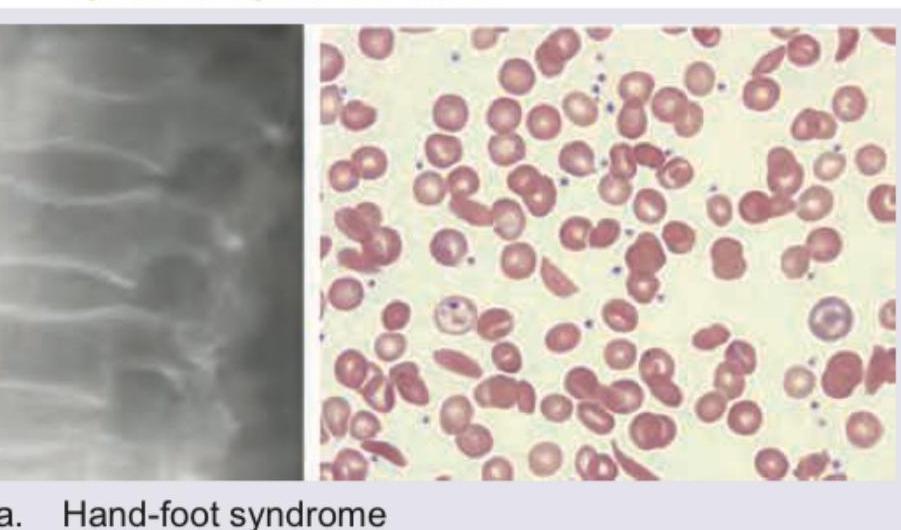
A patient with following peripheral smear and X-ray spine will present with:
Practice by Chapter
Anemia Evaluation and Management
Practice Questions
Hemoglobinopathies
Practice Questions
Thalassemias
Practice Questions
Platelet Disorders
Practice Questions
Coagulation Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Leukemias
Practice Questions
Lymphomas
Practice Questions
Multiple Myeloma and Plasma Cell Disorders
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Transfusion Medicine
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app