
Hematology — MCQs

On this page
Sickle cell anemia leads to resistance towards?
What is used for exchange blood transfusion?
Which of the following statements about Fanconi anemia is false?
Which of the following statements about Hematochromatosis is true?
Mentzer index more than 13 suggests a diagnosis of
Female on carbimazole therapy presents with sudden fever, rigors and sore throat. Which is the investigation of choice for this patient?
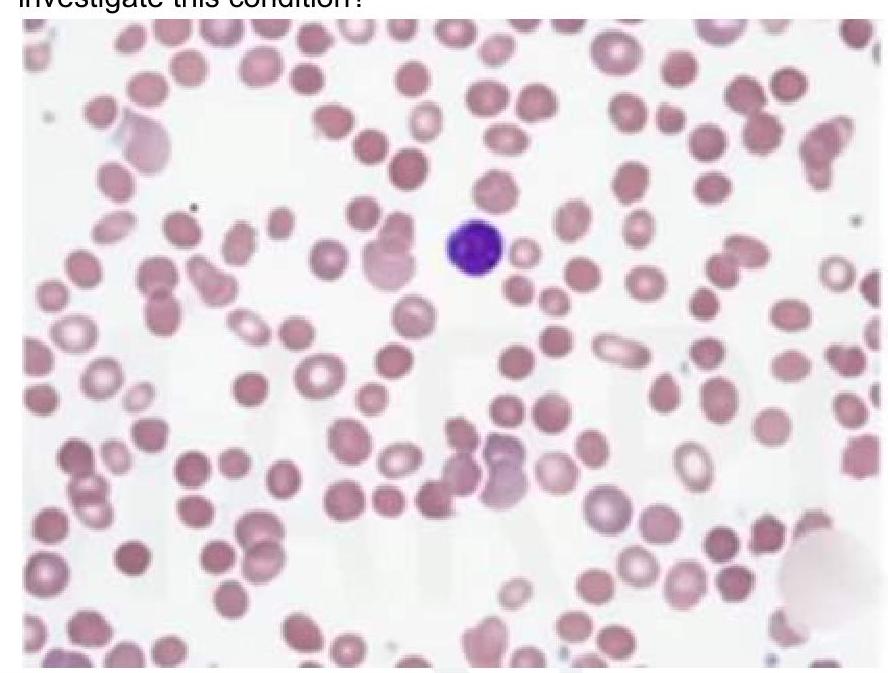
A child presents with intermittent jaundice and splenomegaly. There is a history of similar complaints in the elder brother. Peripheral smear shows the following finding. What is the most appropriate investigation for this condition?
A young patient presents with a large retroperitoneal hemorrhage and a history of intermittent knee swelling after strenuous exercise. There is no history of mucosal bleeding. Which of the following clotting factors is primarily deficient in Hemophilia A?
A female patient presented with fatigue and a history of piles. Routine complete blood count analysis showed hemoglobin of 9 g/dL, MCV 60fL, and RBC count of 5.2 million. A peripheral smear is provided. Which of the following is the next best investigation after the smear for this patient?

A 23-year-old male presented with a history of fatigue and tiredness. On investigation, he was found to have Hb values of 9gm%, MCV of 101 FL. Peripheral smear examination showed hypersegmented neutrophils. Which is the most probable etiology?
Practice by Chapter
Anemia Evaluation and Management
Practice Questions
Hemoglobinopathies
Practice Questions
Thalassemias
Practice Questions
Platelet Disorders
Practice Questions
Coagulation Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Leukemias
Practice Questions
Lymphomas
Practice Questions
Multiple Myeloma and Plasma Cell Disorders
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Transfusion Medicine
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app