
Hematology — MCQs

On this page
A 32-year-old woman presents with fever, fatigue, jaundice, and anemia. Laboratory results show hemoglobin of 7.5, a high reticulocyte count, and elevated indirect bilirubin. The peripheral smear reveals spherocytes. What is the definitive treatment?
In which condition are multiple lytic lesions typically seen?
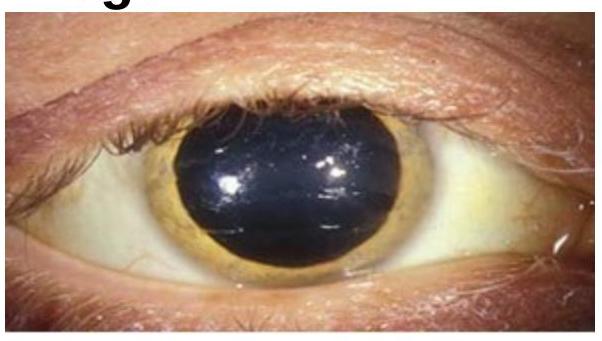
Choose the best method of diagnosis for the clinical sign represented in the image.
What is the first-line treatment for idiopathic thrombocytopenia purpura (ITP)?
Which of the following is typically not associated with secondary Idiopathic thrombocytopenic purpura?
What is the earliest hematological change following splenectomy?
Which of the following statements is false regarding beta thalassemia major?
Treatment of chronic phase of CML in pregnant women is -
Multiple episodes of acute chest syndrome are associated with which of the following conditions?
All of the following statements about Burkitt's lymphoma are true, Except:
Practice by Chapter
Anemia Evaluation and Management
Practice Questions
Hemoglobinopathies
Practice Questions
Thalassemias
Practice Questions
Platelet Disorders
Practice Questions
Coagulation Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Leukemias
Practice Questions
Lymphomas
Practice Questions
Multiple Myeloma and Plasma Cell Disorders
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Transfusion Medicine
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app