
General Medicine — MCQs

On this page
A 60-year-old male with a history of diabetes and hypertension is found unconscious. On examination, his pulse rate is 120/min and BP is 160/100 mm Hg. What is the next step in management?
Smoking is not a risk factor for which of the following conditions?
Deficiency of which complement component is characteristic of Neisseria infection?
Which of the following is true about the therapy of obesity?
In a patient with a smoking history, which factor is most important to assess?
The 'C' wave in the JVP waveform is caused by which of the following events?
20 mEq (mmol) of potassium chloride in 500 ml of 5% dextrose solution is given intravenously to treat which of the following conditions?
The second heart sound (S2) is best appreciated in which of the following areas?
Choose the correct statement(s): 1. Metformin is contraindicated in patients with severe renal impairment (eGFR <30 mL/min/1.73m²) 2. ACE inhibitors should be discontinued immediately if serum creatinine increases by any amount after initiation 3. Beta-blockers are first-line therapy for heart failure with reduced ejection fraction 4. Statins are recommended for primary prevention in patients with diabetes mellitus aged 40-75 years
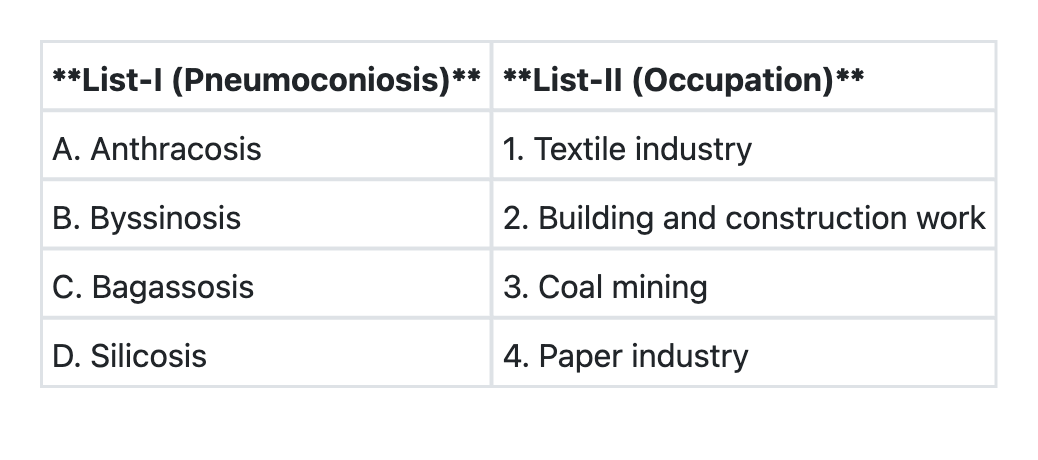
Match List-I with List-II and select the correct answer using the code given below the Lists:
Practice by Chapter
Approach to the Medical Patient
Practice Questions
Differential Diagnosis Development
Practice Questions
Rational Diagnostic Testing
Practice Questions
Medical Decision Making
Practice Questions
Cost-effective Care
Practice Questions
Patient-centered Communication
Practice Questions
Interprofessional Collaboration
Practice Questions
Systems-based Practice
Practice Questions
High-value Care
Practice Questions
Transitions of Care
Practice Questions
Chronic Disease Management
Practice Questions
Medical Uncertainty Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app