
Endocrinology — MCQs

On this page
Prevention or treatment of osteoporosis in post- menopausal women may be achieved by all EXCEPT
A 40 year old lady with temporal field defects and galactorrhoea is most likely to have-
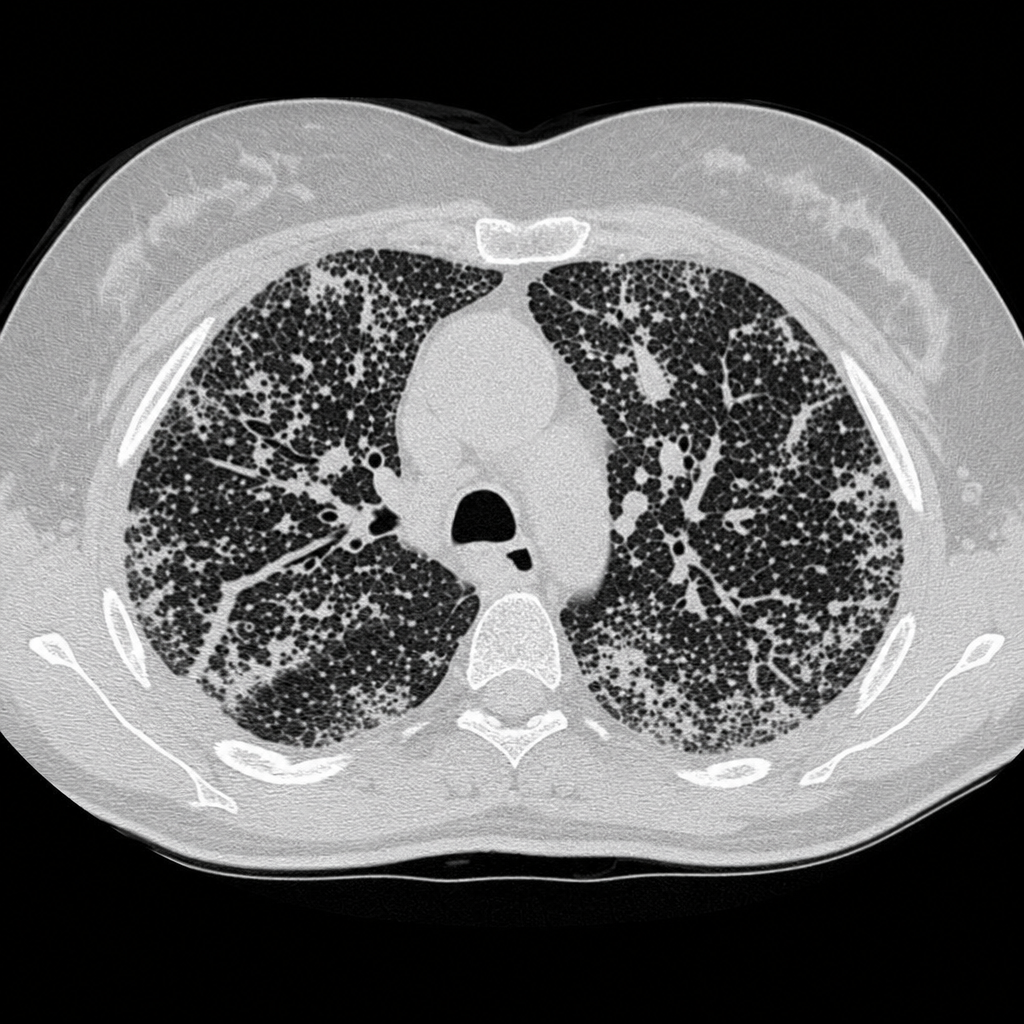
A 30-year-old woman is presented to ER with complaints of progressive lethargy, constipation, muscle weakness, and increased thirst and urination. Lab results confirm hypercalcemia. On further asking, the patient admits taking large doses of calcium and vitamin D supplements on a daily basis. Based on the CT image provided, the metabolic abnormality responsible for her symptoms is also commonly seen in which condition?
True about osteoporosis
A 40-year-old female presents with multiple lytic bone lesions, fracture clavicle and periosteal resorption of 2nd and 3rd metatarsals. What is the most likely diagnosis?
Cerebral salt wasting occurs due to which of the following?
Primary Hyperparathyroidism is associated with -
A 17 years old girl who was evaluated for short height was found to have an enlarged pituitary gland. Her T4 was low and TSH was increased. Which of the following is the most likely diagnosis?
A patient of 47XXY karyotype with features of hypogonadism; likely diagnosis is :
A 24 year old male presents with altered sensorium and rapid shallow breathing. ABG shows:pH 7.2, sodium 140, bicarbonate 10 and chloride 98. Probable diagnosis is -
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app