
Endocrinology — MCQs

On this page
A patient is diagnosed with Cushing Syndrome. What electrolyte imbalance is typically found in this condition?
A patient presents with the clinical findings shown in the image. What is the most appropriate screening test to identify the underlying endocrine condition?

A 25 -year-old presents with weakness, craving for salty foods and postural hypotension. Lab shows serum sodium = 130 mEq/L and serum potassium of 6.0 mEq/L, fasting blood sugar of 65 mg%. All are possible causes of the condition shown except:
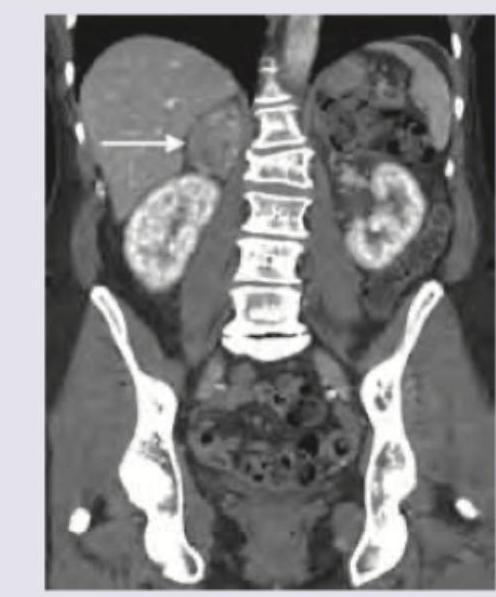
A patient presents with hypertension and hypokalemia, with laboratory findings showing elevated plasma aldosterone and suppressed renin (elevated aldosterone-to-renin ratio). CT abdomen was performed. What is the diagnosis?
All of the following may be associated with the condition shown below except:

All are true about the condition shown except:

A 40-year-old woman with history of progressive shortness of breath has lesions on her legs as shown. HbA1C of the patient is 5.8%. Lipid profile shows serum cholesterol 175 mg%. What is the diagnosis? (Recent NEET Pattem 2016-17)

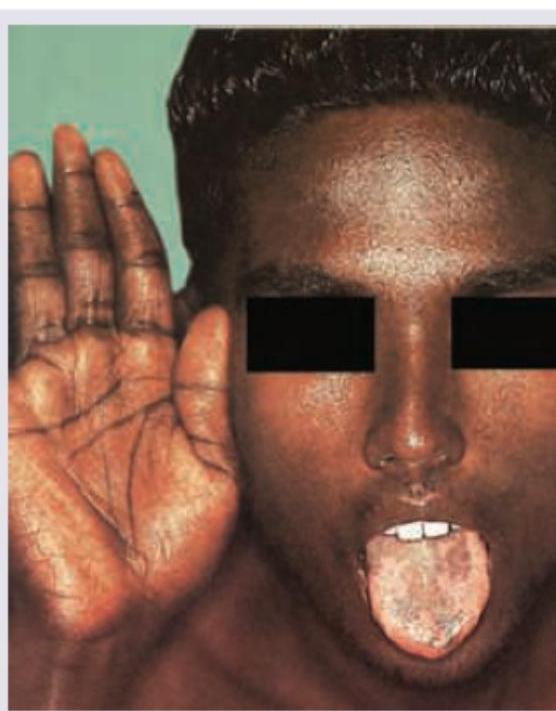
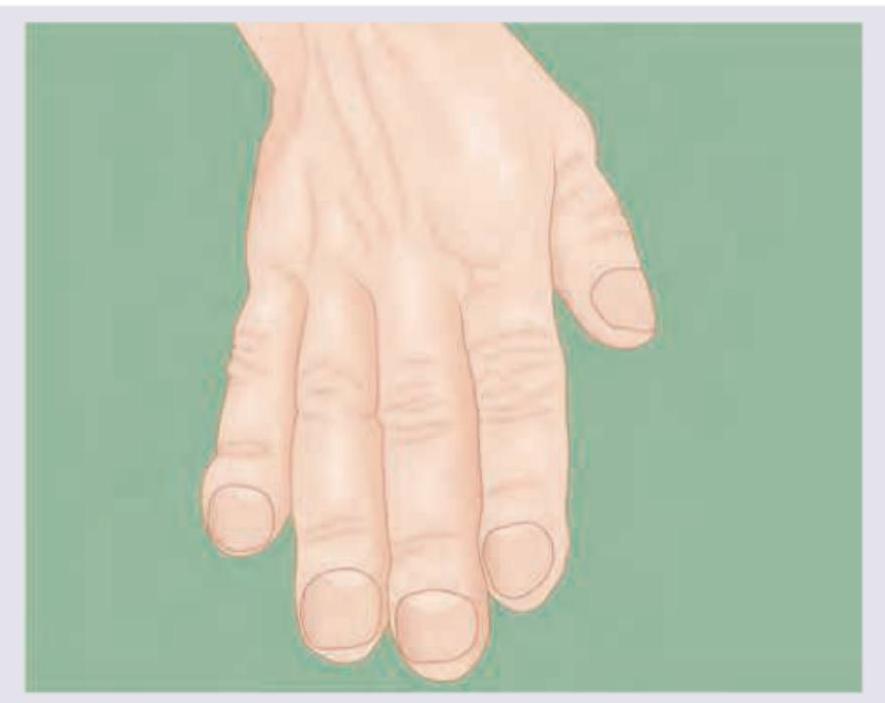
A 50-year-old man presents with frontal bossing, enlarged tongue and following appearance of hand. Which of the following tests should be done in this patient?
Comment on the diagnosis of the image shown below. (AIIMS Nov 2017)

A 68-year-old postoperative patient who has undergone thyroidectomy presents with muscle cramps. ECG shows?
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app