
Endocrinology — MCQs

On this page
A 28-year-old female presents with palpitations, heat intolerance, weight loss of 8 kg over 3 months, and tremors. Examination reveals diffuse thyroid enlargement, exophthalmos, and pretibial myxedema. Thyroid function tests show TSH <0.01 mIU/L, free T4 28 ng/dL (normal 5-12), and free T3 elevated. TSH receptor antibodies are positive. What is the most appropriate definitive treatment?
A 30-year-old man develops an increase in shoe size with coarse facies and large hands. IGF1 is elevated. What is the investigation of choice?
A 56-year-old diabetic patient is currently on Metformin and Insulin Glargine. His HbA1c is 8.2 %, indicating suboptimal glycemic control. Echocardiography reveals a reduced ejection fraction (EF) of 35 %. Which of the following is the most appropriate agent to add to his current regimen?
A known type 1 diabetic presents with glucose 799 mg/dL, Na+ 128 mEq/L, Cl- 88 mEq/L, and signs of dehydration. Which of the following is NOT used in the initial management?
A patient presents with salt wasting, craving, hyperkalemia, metabolic acidosis, and skin pigmentation. What is the most likely diagnosis?
A 60-year-old patient presents with pain in multiple bones and a history of increased hat size. On examination, some bones feel warm to touch. Biochemical investigations show normal serum calcium, phosphate, and parathyroid hormone (PTH) levels, but markedly elevated alkaline phosphatase (ALP). What is the most likely diagnosis
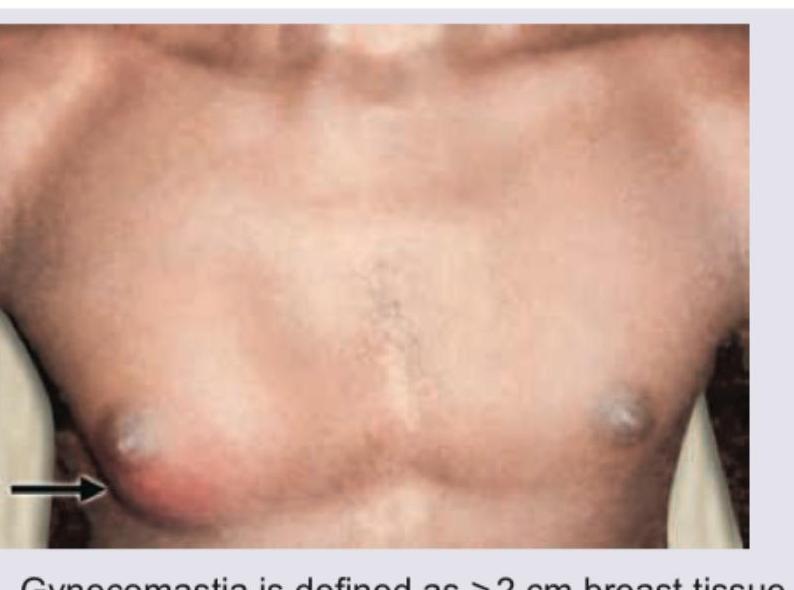
All are true regarding this picture of 16-year-old boy except: (Recent NEET Pattern 2016-17)
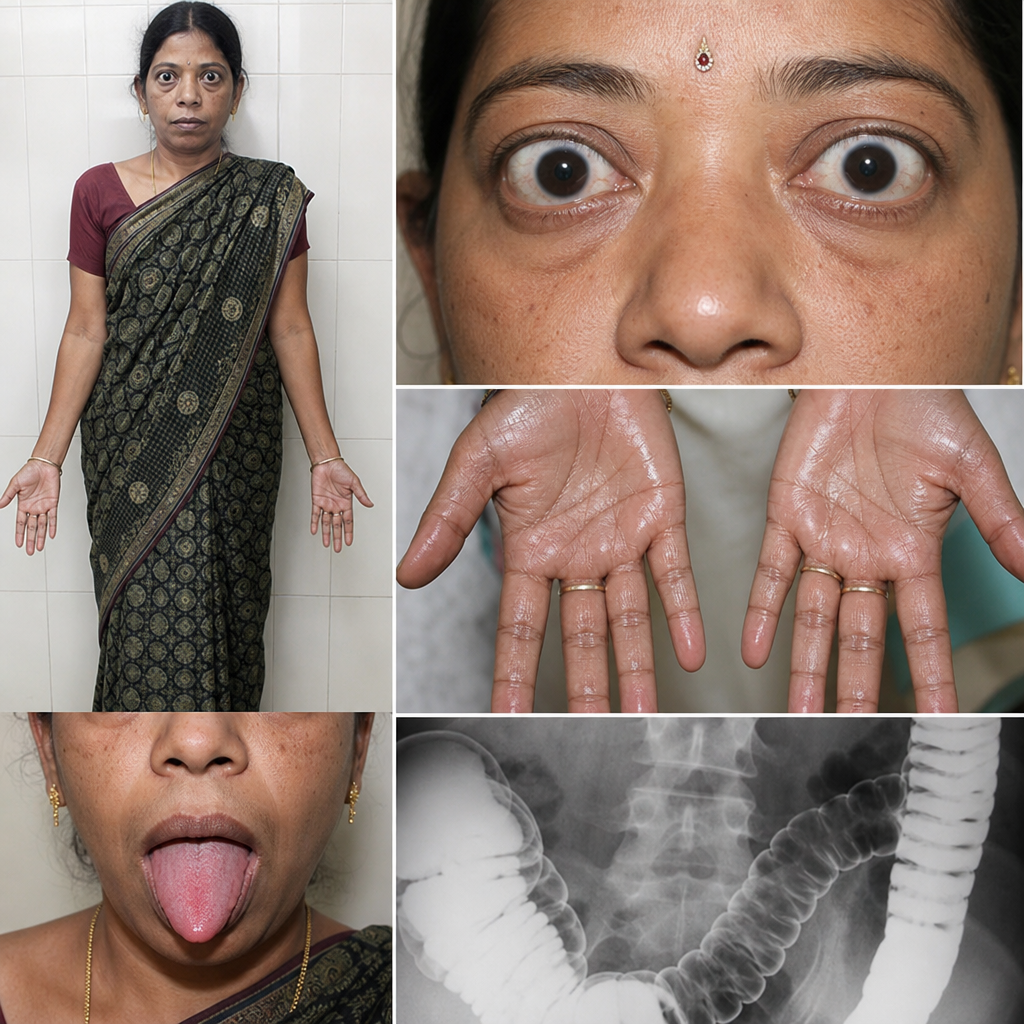
All can be seen in this patient except:
A specific clinical sign is characterized by spasm of hand muscles upon inflating a blood pressure cuff. What is this sign called?
What is the primary hyperaldosteronism due to an adrenal adenoma called?
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app