
Endocrinology — MCQs

On this page
Which of the following is NOT a feature of Kallmann syndrome?
All of the following are helpful in the initial treatment of severe hypercalcemia associated with hyperparathyroidism except?
A patient underwent bilateral adrenalectomy for bilateral pheochromocytoma. One day later, the patient developed lethargy, fatigue, low blood pressure, and a normal pulse. There are no signs of volume deficit. What is the likely course?
A child presents with features of hyperparathyroidism. All of the following are true regarding this condition except:
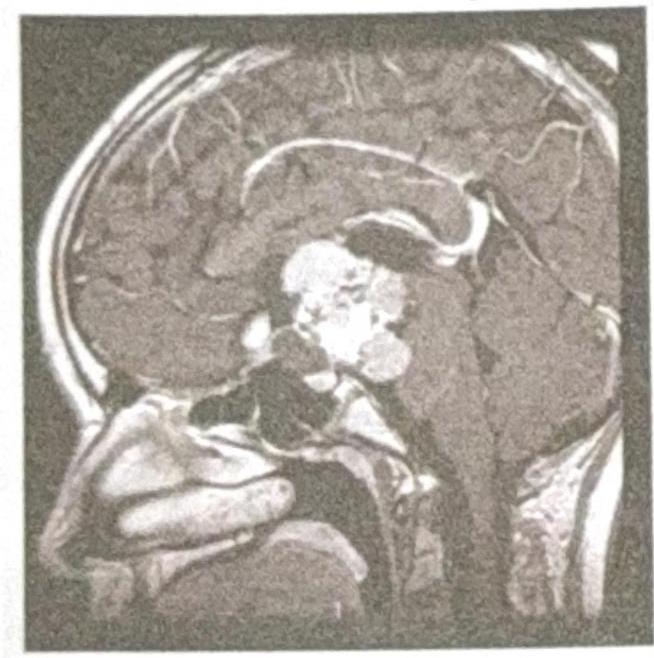
A 39-year-old man presents to his physician with the complaint of loss of peripheral vision. The subsequent magnetic resonance imaging (MRI) scan demonstrates what abnormality?
What is the most common cause of hyperthyroidism?
Diabetes control is best monitored by?
A 40-year-old non-alcoholic male patient presented with jaundice, lethargy, arthralgia, skin pigmentation, loss of libido, polyuria, polydipsia, and exertional dyspnea. On examination, hepatosplenomegaly, increased pigmentation, spider angiomas, arthropathy, ascites, loss of body hair, and testicular atrophy were noted. Liver function tests were deranged, and insulin levels were raised. Liver biopsy was performed. The patient had no history of long-term medication intake. Iron studies revealed: Plasma iron - 200 microgm/dL, TIBC - 300 microgm/dL, Transferrin saturation - 90%, Serum ferritin - 5000 microgm/L, Liver iron - 10000 microgm/gm of dry weight, Hepatic iron index - 3. What is the most common mutation seen in this condition?
All of the following are features of acromegaly, except?
Hypoglycemia is an important feature of which of the following conditions?
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app