
Endocrinology — MCQs

On this page
Which of the following is seen in secondary hyperparathyroidism?
A couple has two children and is currently unable to conceive. The father is diagnosed with hypogonadotropic hypogonadism. Which of the following statements is false regarding his condition?
A patient presents with increased serum calcium and decreased serum phosphate. What is the most likely diagnosis?
What is true about thyroid storm?
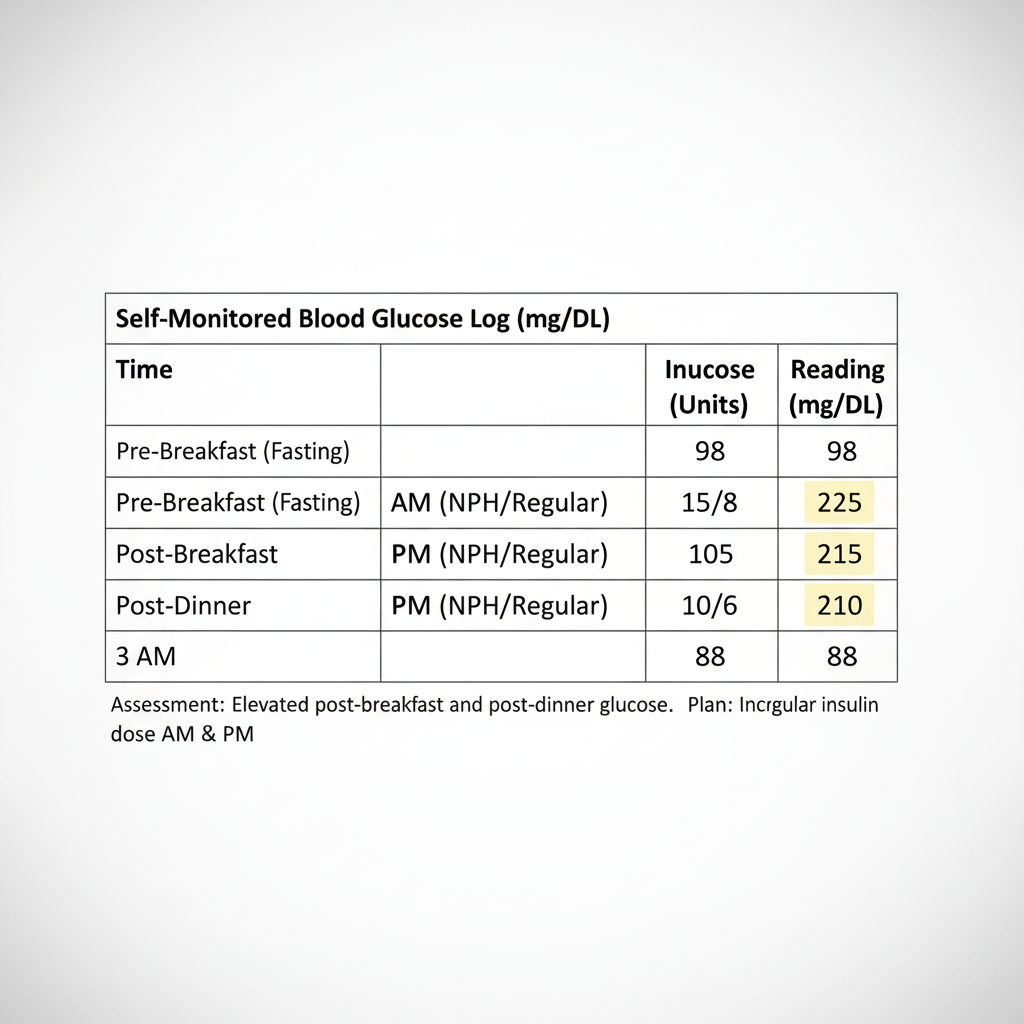
A patient with IDDM injects a mixture of NPH insulin and crystalline zinc (Regular) insulin before breakfast (at 7 AM) and before dinner (at 8 PM) each day. She reports the following average self-monitored RBS for the past week. | Time of Reading | Glucose (mg/dL) | Insulin Dose (Units) | |---|---|---| | Pre-Breakfast (Fasting) | 95 | NPH 10 / Regular 6 (7 AM) | | Post-Breakfast | 220 | — | | Pre-Dinner | 100 | NPH 8 / Regular 5 (8 PM) | | Post-Dinner | 215 | — | | 3 AM | 90 | — |
A patient presents with polyuria and elevated prolactin levels. There is a family history of the father dying due to renal stones. The patient has a Ca2+ of 12 g% and PTH levels of 260 IU/L. What is the most likely diagnosis?
Which one of the following is NOT an appropriate treatment for hyperthyroidism due to subacute lymphocytic thyroiditis?
A 14-year-old boy presents with a 3-month history of increasing weakness, easy fatigability, and weight loss. He also reports recent onset of nausea, vomiting, and abdominal pain. His blood pressure is markedly decreased, and he has increased pigmentation of his skin creases. What is the most likely diagnosis?
What is the most characteristic symptom in a patient diagnosed with Pheochromocytoma?
Acromegaly is associated with all of the following EXCEPT:
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app