
Endocrinology — MCQs

On this page
Anti-thyroglobulin antibodies are seen in which of the following conditions?
What is the most common malignancy of the endocrine system?
A 40-year-old woman presents with an 8-month history of severe headaches, weakness, and dizziness. Her blood pressure is 180/110 mm Hg. Physical examination shows diminished tendon reflexes. An abdominal CT scan reveals a 4-cm mass in the right adrenal gland. Laboratory studies include serum potassium of 2.3 mEq/L, serum sodium of 155 mEq/L, plasma cortisol of 25 mg/dL (8 AM) and 20 mg/dL (4 PM), and low plasma renin. These clinical and laboratory findings are consistent with an adrenal tumor that secretes which of the following hormones?
Hypercalcemia would not be expected to occur as a result of which of the following conditions?
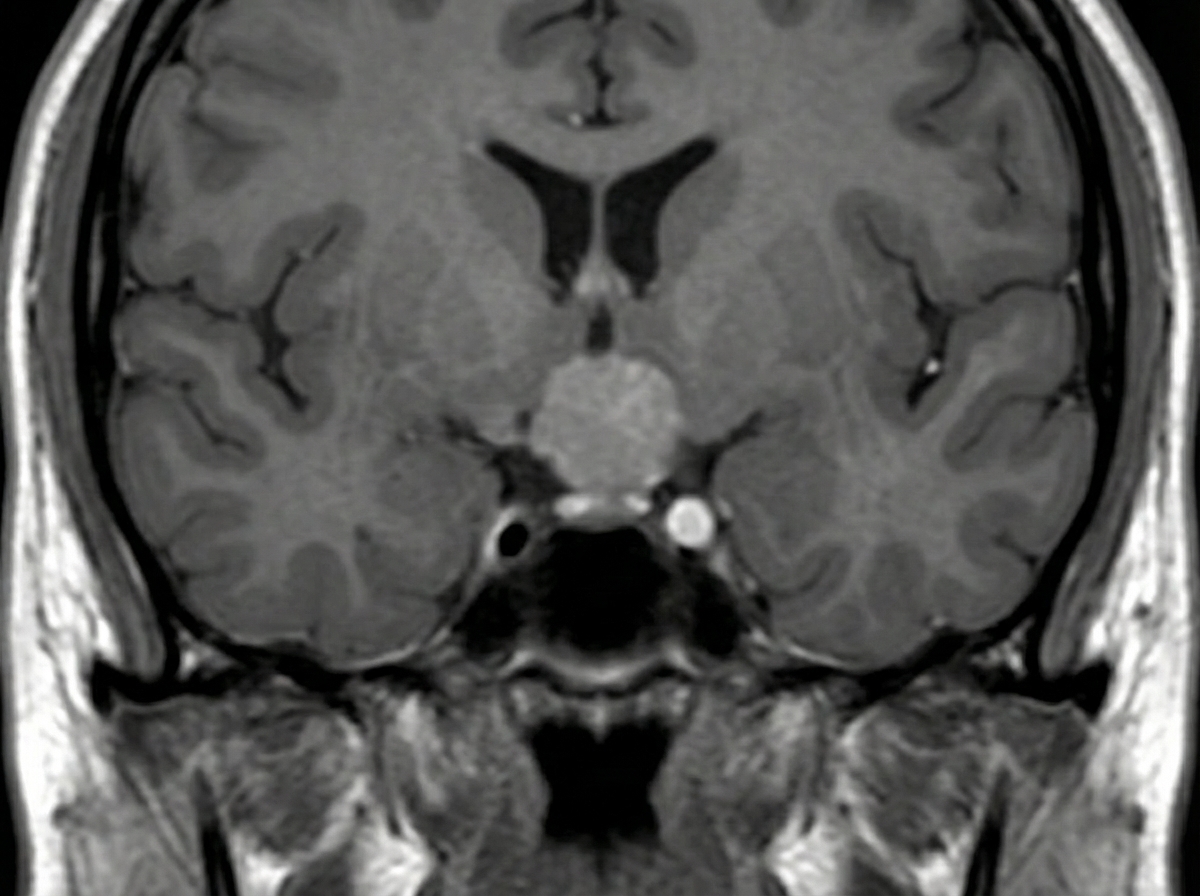
A 34-year-old man presents with a chief complaint of blurring of vision in both eyes and headache for the past six months, accompanied by decreased libido. Examination reveals bitemporal hemianopia. An MRI was performed. What is the most likely diagnosis?
Which of the following conditions can cause hypoglycemia, except?
The syndrome of inappropriate antidiuretic hormone (SIADH) is characterized by which of the following findings?
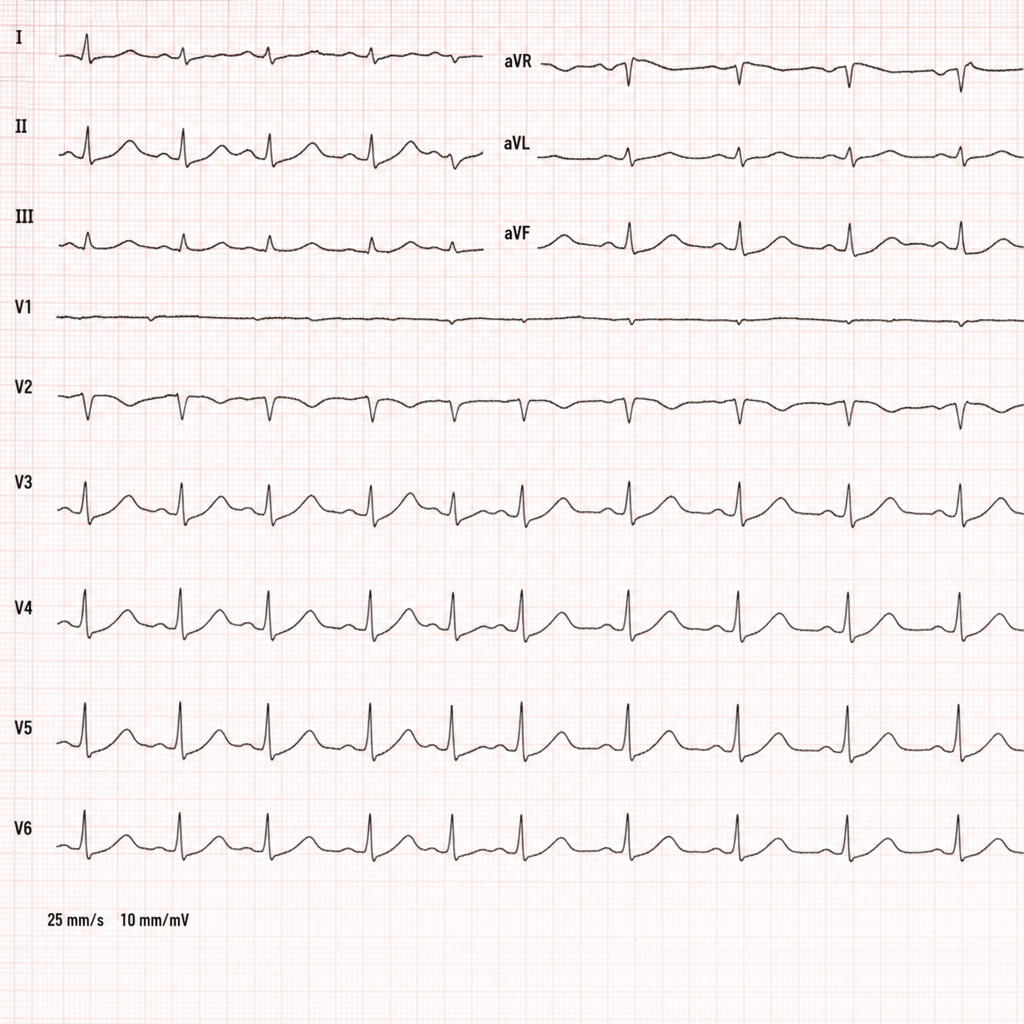
A young lady was found unconscious while exercising. Her blood glucose was 250 mg/dL with metabolic acidosis on ABG, and no prior history of diabetes. DKA was diagnosed and managed. Her ECG is shown. Where is the pathology likely located in the heart of the patient in this clinical scenario?
A 37-year-old woman presents with a one-week history of difficulty swallowing and a feeling of fullness in the anterior neck. She had a mild upper respiratory tract infection one month prior. On examination, her temperature is 37.4°C, pulse is 74/min, respirations are 16/min, and blood pressure is 122/80 mm Hg. Palpation of her diffusely enlarged thyroid is painful. Laboratory studies reveal an increased serum T4 level and a decreased TSH level. Two months later, her symptoms have resolved, and her T4 level is normal. Which of the following conditions is most likely to have produced these findings?
Manifestations of endemic cretinism include:
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app