
Endocrinology — MCQs

On this page
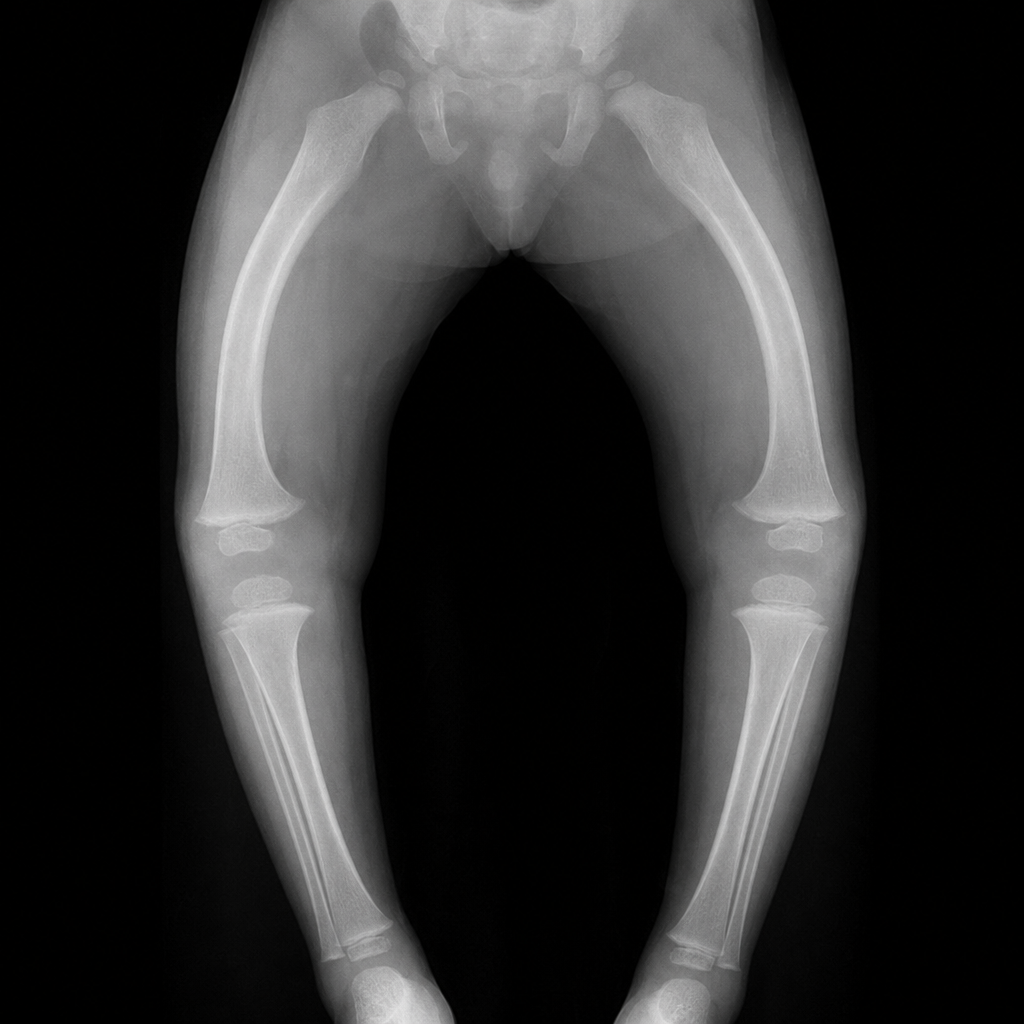
A 72-year-old man presents with progressive bone pain in his right leg and skull. He reports increasing hat size over the past few years. On examination, there is bowing of the right tibia and warmth over the affected bone. A radiograph of the right tibia shows cortical thickening, coarsened trabecular pattern, and a 'blade of grass' lytic lesion advancing along the shaft — findings consistent with Paget's disease of bone. Which one of the following biochemical measures would be most likely to be elevated in this patient?
Which of the following is NOT a cardiovascular finding in an elderly patient with thyrotoxicosis?
Gynecomastia is not associated with which of the following?
What is the best initial advice to be given to a patient newly diagnosed with type 2 Diabetes Mellitus?
A 30-year-old nurse is evaluated for recurrent hypoglycemia. She feels shaky, anxious, and sweaty; her plasma glucose is 50 mg/dl during an attack at work. She then drinks coffee and feels better. These episodes have not happened outside the work environment. She takes no medications and is otherwise healthy. Which is the most appropriate diagnostic test in this patient?
A 42-year-old patient presents with obesity, glucose intolerance, hypertension, alkalosis, and proximal myopathy. Her ACTH levels did not drop after administering steroids. What is the diagnosis?
What percentage of pheochromocytomas are malignant?
Ectopic ACTH syndrome is most commonly associated with which of the following conditions?
In Multiple Endocrine Neoplasia type I (MEN I), which of the following tumors is seen most commonly?
A hand radiograph shows subperiosteal cortical resorption along the radial aspects of the middle phalanges. Which of the following conditions is most likely associated with this finding?

Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app