
Endocrinology — MCQs

On this page
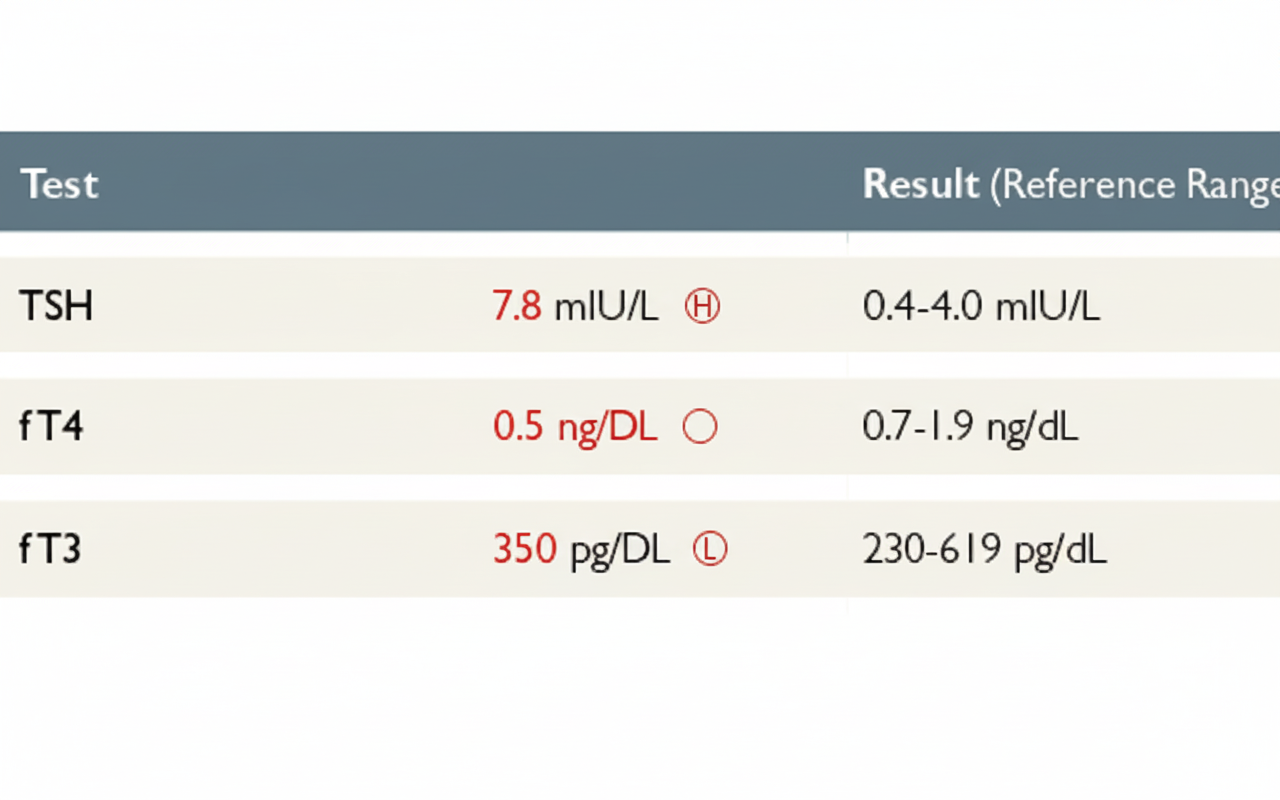
The laboratory investigation of a patient shows T4 and TSH levels. Which of the following is the most likely diagnosis?
A diabetic patient in the waiting room develops giddiness, sweating, and confusion. What is the most likely condition?
Diabetic ketoacidosis (DKA) mimics acute pancreatitis in all the following findings except?
A 55-year-old obese woman presents with frequent vaginal yeast infections in the past 2 months, recent weight loss despite a large appetite, and nocturia. She has a history of hypertension treated with ramipril. What is the most likely diagnosis?
Which of the following is the LEAST likely symptom of hyperthyroidism in a 77-year-old man?
Which of the following obesity-related syndromes is associated with hypogonadism in males but not in females?
A child underwent bilateral adrenalectomy. Later, the child developed headache, visual field defect, and hyperpigmentation of the skin. What is the most probable diagnosis?
All of the following are true of cerebral salt wasting syndrome, except:
Which of the following is NOT a primary cause of hypogonadism?
A 40-year-old female presenting with intolerance to cold, constipation, and hoarseness of voice was found to have cardiomegaly on chest roentgenogram. Which of the following investigations is the best to determine the cause of her cardiomegaly?
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app