
Endocrinology — MCQs

On this page
Most common hormone deficiency that occurs after intracranial irradiation is
Commonest cause of hypothyroidism is
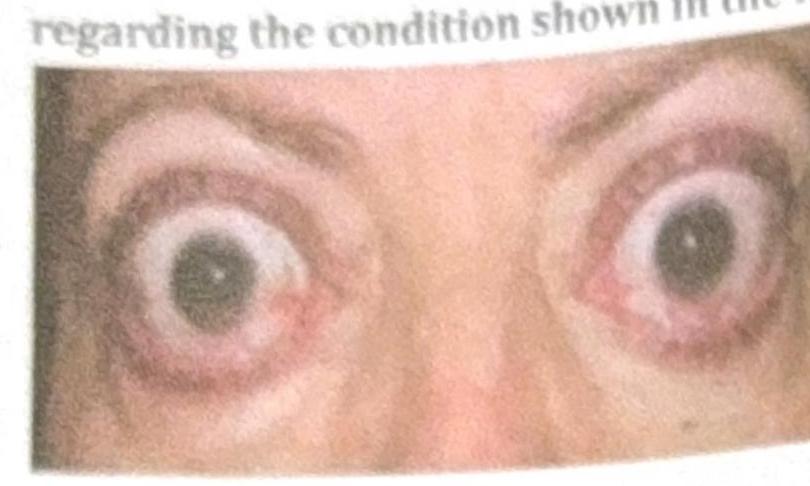
Which of the following statements about thyroid eye disease is false?
A 30-year-old woman presents with a history of amenorrhea and impaired vision of six months' duration. Physical examination shows normal findings except for pale optic discs and diminished visual acuity. The most likely diagnosis is -
The tumor which is more commonly located in the tail of the pancreas is:
In Osteoporosis which of these is seen?
Pendred's syndrome is:
Slow relaxation of tendon reflexes may be a manifestation of:
Osteomalacia is due to -
Prevention or treatment of osteoporosis in post- menopausal women may be achieved by all EXCEPT
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app