
Endocrinology — MCQs

On this page
A 28-year-old female presents with panic attacks, palpitations, sweating, and chest pain. EKG shows sinus tachycardia. Labs reveal decreased TSH and increased FT4. Analyze and choose the most likely diagnosis.
A 38-year-old woman presents with visual field defects and galactorrhea. An MRI reveals a pituitary mass. Which class of drugs would be most appropriate for treating this condition?
A 45-year-old woman presents with fatigue, dry skin, and constipation. Physical examination reveals a delayed relaxation phase of deep tendon reflexes. Laboratory tests show elevated TSH and low free T4. What is the most likely diagnosis?
A 65-year-old woman with a history of hyperthyroidism presents with fever, tachycardia, and confusion. What is the most likely diagnosis?
What are the endocrine and autoimmune mechanisms involved in a 55-year-old female presenting with palpitations, tremors, weight loss, high free T4, and low TSH?
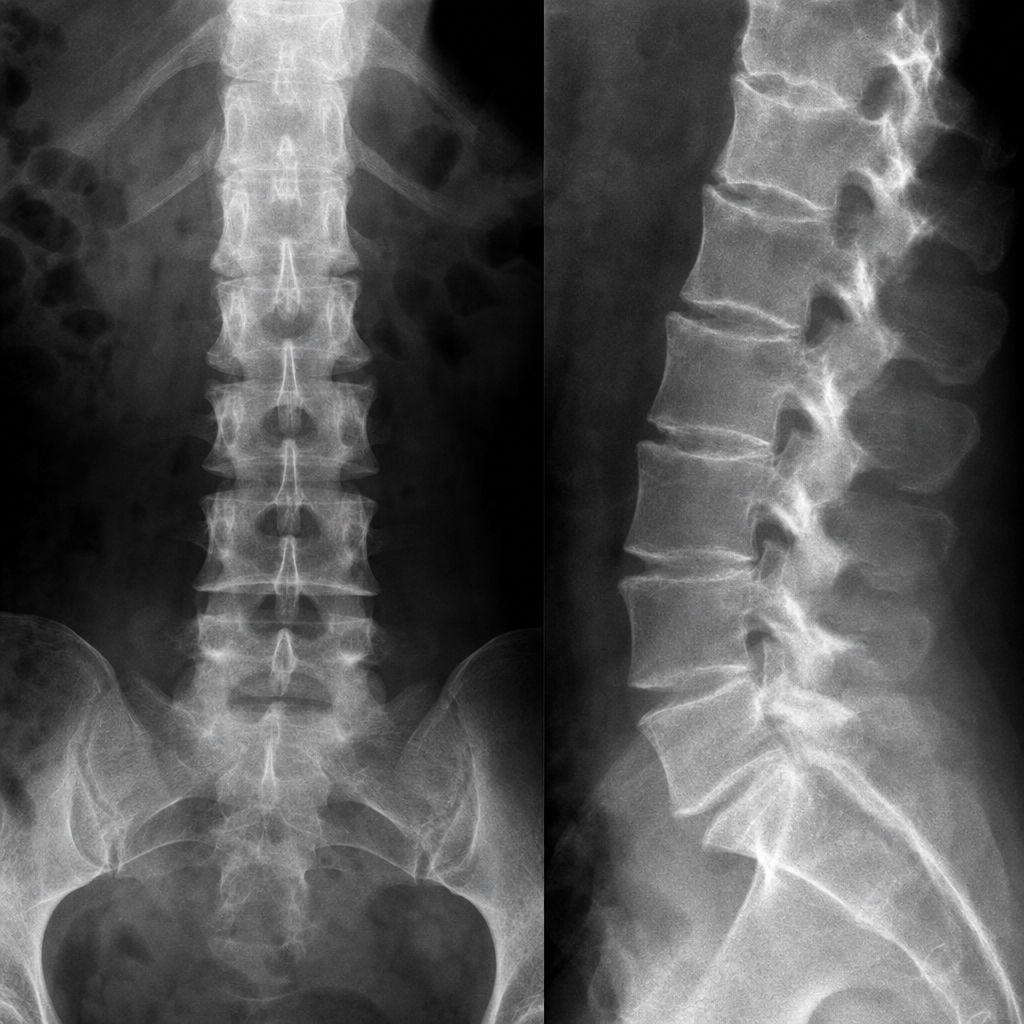
What is the diagnosis of a 55-year-old woman with chronic low backache?
What is the primary pathophysiological consequence of Graves' disease?
In which condition would elevated calcium levels be most likely to occur, potentially triggering calcitonin secretion?
In which condition is radioiodine preferred for treatment?
Which of the following conditions is least likely to be associated with osteoporosis?
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app